Factors That Can Affect Ingestive Behaviour: Psychological or Hedonic Factors
 Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour:
Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour:
Psychological or Hedonic Factors
In contrast to hyperphagia resulting from physical hunger, over‐eating for emotional reward or as a coping strategy is regulated by the hedonic system and has little to do with the body’s real or perceived need for calories. The range of psychological or emotional factors that can initiate and influence eating encompass virtually the entire range of emotional responses including stress, frustration, loneliness, anxiety, anger, disgust, fear, grief, joy, relief, all of which can significantly alter dietary restraint or promote disinhibition. Typically, hedonic hyperphagia is associated with the selection and consumption of highly palatable energy‐dense ‘comfort’ foods, although homeostatic hyperphagia also tends to be associated with the preferential consumption of palatable foods.
In addition to simple ‘emotional’ over‐eating, specific psychiatric conditions that affect food intake or can pose important barriers to maintaining a healthy diet must be considered. Increased appetite is a feature of atypical depression and can be interpreted as ‘self‐medicating’ with food – particularly in cases where these foods affect the serotonergic and reward systems to improve mood. Binge eating, night eating and other abnormal eating behaviours must also be seen in the context of underlying emotional or psychological processes that are distinct from homeostatic ingestive behaviour. Other mental health conditions that can significantly affect eating include attention deficit disorders, post‐traumatic stress syndrome, sleep disorders, chronic pain, anxiety disorders, addictions, seasonal affective disorder and cognitive disorders. Particularly sleep deprivation has been associated with increased appetite and ingestion of highly palatable snacks as well as increased risk for diabetes. Patients with obesity resulting from emotional eating or hedonic hyperphagia are most likely to benefit more from psychological and/or psychiatric interventions rather than simply from dietary counselling.
Commentary: Although for didactic and practical purposes I find it helpful to distinguish between what I have referred to as “homeostatic” vs. “hedonic” hyperphagia, it is important to note that at a physiological level, the distinction between the “homeostatic” and “hedonic” pathways is not as clear cut as is often assumed. In fact, there is close and complex cross talk between these pathways. For example, hunger, a feature of the “homeostatic” pathway, is also a powerful activator of the “hedonic” pathway, thus leading to seeking out and consumption of caloric-dense foods. On the other hand, “hedonic” drivers to eat can override satiety and lead to eating even when not hungry. This, physiology, however, does not take away from the fact that in clinical evaluation, trying to distinguish between homeostatic and hedonistic is often helpful in determining the appropriate treatment path.
@DrSharma
Edmonton, AB
How The Body Weighs Itself – Evidence For A Bone “Gravitostat”
 In my talks, I have often joked about how to best keep weight off – just carry around a backpack that contains the lost pounds to fool the body into thinking the weight is still there.
In my talks, I have often joked about how to best keep weight off – just carry around a backpack that contains the lost pounds to fool the body into thinking the weight is still there.
It turns out that what was intended as a joke, may in fact not be all too far from how the body actually regulates body weight.
As readers of these posts are well aware, body weight is tightly controlled by a complex neuroendocrine feedback system that effectively defends the body against weight loss (and somewhat, albeit less efficiently, protects against excessive weight gain).
Countless animal experiments (and human observations) show that following weight loss, more often than not, body weight is regained, generally precisely to the level of initial weight.
With the discovery of leptin in the early 90s, an important afferent part of this feedback system became clear. Loss of fat mass leads to a substantial decrease in leptin levels, which in turn results in increased appetite and decreased metabolic rate, both favouring weight regain and thus, restoration of body weight to initial levels.
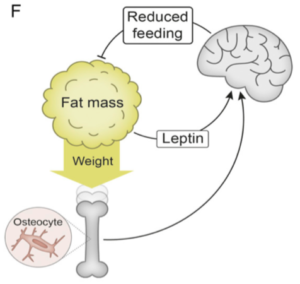
Now, an international team of researchers led by John-Olov Jansson from the University of Gothenburg, Sweden, in a paper published in the Proceeding of the National Academy of Science (PNAS), provides compelling evidence for the existence of another afferent signal involved in body weight regulation – one derived from weight-bearing bones.
Prompted by observations that prolonged sedentariness can promote weight gain, independent of physical activity, the researchers hypothesised that,
“…there is a homeostat in the lower extremities regulating body weight with an impact on fat mass. Such a homeostat would (together with leptin) ensure sufficient whole body energy depots but still protect land-living animals from becoming too heavy. A prerequisite for such homeostatic regulation of body weight is that the integration center, which may be in the brain, receives afferent information from a body weight sensor. Thereafter, the integration center may adjust the body weight by acting on an effector.”
In a first series of experiments, the researchers observed that implanting a weight corresponding to about 15% of body weight into rodents (rats and mice), resulted in a rapid “spontaneous” adjustment in body weight so that the combined weight of the animal plus the weight implant corresponded more-or-less to that of control animals.
Within two weeks of implanting the weights, ∼80% of the increased loading was counteracted by reduced biological weight, largely due to reduced white adipose tissue (WAT), accompanied by a corresponding decrease in serum leptin levels. (Interestingly, this weight loss was also accompanied by a substantial improvement in insulin resistance and glucose homeostasis).
The decrease in “biological” body weight was mainly attributable to a reduction in caloric intake with no changes in fat oxidation, energy expenditure or physical activity.
Removal of the implanted weights resulted in rapid weight regain to initial levels, showing that the “weight sensor” was active in both directions.
Experiments showed that this “weight sensing” mechanism was largely independent of the leptin pathway and did not appear to involve grehlin, GLP-1, a-MSH, estrogen receptor-a, or the sympathetic nervous system.
Now for the interesting part: the observed effect of weight loading was not seen in mice depleted specifically of DMP1 osteocytes, demonstrating that the suppression of body weight by loading is dependent on osteocytes.
As the authors note, these findings are consistent with a growing body of data indicating that the skeleton is an endocrine organ that regulates energy and glucose metabolism. Indeed, it is well known that osteocytes can sense dynamic short term high-impact bone loading for local bone adaptation – now it appears, that osteocytes may also play a vital role in sensing overall body weight and signalling this to the brain centres that regulate energy balance and body weight.
Thus, in summary, not only have the authors provided compelling evidence for a “weight-sensing” role for bone osteocytes (presumably through their presence in the long weight-bearing bones of our lower extremities) but also provide a plausible biological explanation for the weight gain and change in fat mass seen with prolonged sedentariness (which literally takes the weight off the bone).
These findings may also finally explain why rats held at increased gravity for extended periods of time (simulated G2) become lean even when their energy intake matches their expenditure.
Perhaps, carrying around a heavy backpack may indeed help with long-term weight loss maintenance after all – who knew?
@DrSharma
Berlin, D
Hat tip to Jean-Philippe Chaput for alerting me to this article
The Key To Obesity Management Lies In The Science Of Energy Homeostasis
 If there is one thing we know for sure about obesity management, it is the sad fact, that no diet, exercise, medication, not even bariatric surgery, will permanently reset the body’s tendency to defend and regain its body weight to its set point – this generally being the highest weight that has been achieved and maintained for a notable length of time.
If there is one thing we know for sure about obesity management, it is the sad fact, that no diet, exercise, medication, not even bariatric surgery, will permanently reset the body’s tendency to defend and regain its body weight to its set point – this generally being the highest weight that has been achieved and maintained for a notable length of time.
Thus, any effective long-term treatment has to offset the complex neurobiology that will eventually doom every weight-loss attempt to “failure” (no, anecdotes don’t count!).
Just how complex and overpowering this biological system that regulates body weight is, is described in a comprehensive review by the undisputed leaders in this field (Michael Schwartz, Randy Seeley, Eric Ravussin, Rudolph Leibel and colleagues) published in Endocrine Reviews. Indeed the paper is nothing less than a “Scientific Statement” from the venerable Endocrine Society, or, in other words, these folks know what they’re talking about when it comes to the science of energy balance.
As the authors remind us,
“In its third year of existence, the Endocrine Society elected Sir Harvey Cushing as President. In his presidential address, he advocated strongly in favor of adopting the scientific method and abandoning empiricism to better inform the diagnosis and treatment of endocrine disease. In doing so, Cushing helped to usher in the modern era of endocrinology and with it, the end of organo-therapy. (In an interesting historical footnote, Cushing’s Energy Homeostasis and the Physiological Control of Body-Fat Stores presidential address was given in , the same year that insulin was discovered.)”
Over 30 pages, backed by almost 350 scientific citations, the authors outline in excruciating detail just how complex the biological system that regulates, defends, and restores body weight actually is. Moreover, this system is not static but rather, is strongly influenced and modulated by environmental and societal factors.
Indeed, after reading this article, it seems that the very notion, that average Jane or Joe could somehow learn to permanently overcome this intricately fine-tuned system (or the societal drivers) with will power alone is almost laughable (hats off to the very few brave and determined individuals, who can actually do this – you have climbed to the top of Mount Everest and decided to camp out there for the foreseeable future – I wish you all the best!).
Thus, the authors are confident that,
“The identification of neuromolecular mechanisms that integrate short-term and long-term control of feeding behavior, such that calorie intake precisely matches energy expenditure over long time intervals, will almost certainly enable better preventive and therapeutic approaches to obesity.”
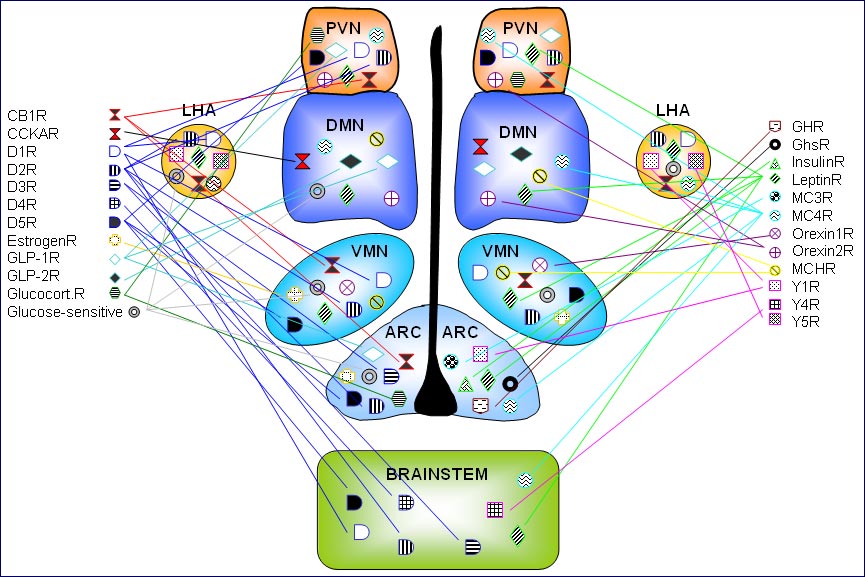
Sadly, despite all we have learnt about this system, we are still far from fully understanding it. Thus, the canonical molecular/ cellular signaling pathway: LEP → LEPR → POMC, AgRP → PC → MC4R is just one pathway in a complex network of multiple interacting and sometimes redundant pathways that involve virtually every part of the brain.
Also, the effect of environmental factors appears to be far more complex than most people think. Thus,
“During sensitive periods of development, ontogenic processes in both brain and peripheral organs can be modified so as to match anticipated environmental conditions. Although many exposures during development could potentially predispose to obesity in adulthood, we focus here on two that some researchers think contribute to the secular trends in obesity: parental obesity and exposure to endocrine disrupting chemicals (EDCs).”
Throw in the role of gut bugs, infections, and societal factors, and it is easy to see why no simple solution to the obesity epidemic are in sight (let alone a range of effective long-term treatments like we have for most other common chronic diseases).
As for solutions,
“To be viable, theories of obesity pathogenesis must account not only for how excess body fat is acquired, but also for how excess body fat comes to be biologically defended. To date, the preponderance of research has focused on the former. However, we must consider the possibility that some (perhaps even most) mechanisms underlying weight gain are distinct from those responsible for the biological defense of excess fat mass. A key question, therefore, is how the energy homeostasis system comes to defend an elevated level of fat mass (analogous to the defense of elevated blood pressure in patients with hypertension). Answering this question requires an improved understanding of the neuro-molecular elements that underlie a “defended” level of body fat. What are the molecular/neuroanatomic predicates that help establish and defend a “set point” for adiposity? How do these elements regulate feeding behavior and/or energy expenditure, so as to achieve long-term energy balance? By what mechanisms is an apparently higher set point established and defended in individuals who are obese?” [sic]
Clearly,
“Given that recovery of lost weight (the normal, physiological response to weight loss irrespective of one’s starting weight) is the largest single obstacle to effective long-term weight loss, we cannot overstate the importance of a coherent understanding of obesity-associated alterations of the energy homeostasis system.”
There is much work to be done. Whether or not, in this climate of anti- and pseudo-science, funding for such fundamental work will actually be made available, is anyone’s guess.
@DrSharma
Edmonton, AB
Zona Incerta Stimulation Provokes Instant Binge Eating in Mice
 The neuronal control of appetite and food intake is among the most complex and fascinating systems.
The neuronal control of appetite and food intake is among the most complex and fascinating systems.
Now, in a paper published in Science, Xiaobing Zhang and Anthony van den Pol from Yale University, New Haven, report the identification of a novel role of the zona incerta in inducing profound binge eating behaviour in mice.
The zona incerta, is a little know part of the central nervous system within the subthalamus with extensive projections all the way from the cerebral cortex into the spinal cord. It is thought to play an important role in limbic-motor integration as well as synchronizing brain rhythms.
The researchers showed that optogenetic stimulation of zona incerta GABA neurons or their axonal projections to paraventricular thalamus excitatory neurons rsults in an immediate (in 2 to 3 seconds) binge-like eating behaviour – the animals ate up to 35% of their total energy requirements in just 10 mins.
Furthermore, while intermittent stimulation of these neurons led to body weight gain, ablation reduced weight.
The authors suggest that the identification of this novel orexigenic system may lead to better treatments not just for binge-eating disorder.
@DrSharma
Edmonton, AB
POMC Mutation Obesity Responds To Melanocortin-4 Receptor Agonist
 Melanocyte-stimulating hormone (a-MSH), which is produced from the hormone precursor proopiomelanocortin (POMC) and acts on the hypothalamic melanocortin-4 receptor, plays a key role in the regulation of satiety and energy expenditure.
Melanocyte-stimulating hormone (a-MSH), which is produced from the hormone precursor proopiomelanocortin (POMC) and acts on the hypothalamic melanocortin-4 receptor, plays a key role in the regulation of satiety and energy expenditure.
In very rare instances, mutations of the gene coding for POMC can cause severe early onset obesity characterised by increased appetite. Due to other effects of POMC deficiency, patients will present with pale skin, red hair and clinical signs of hypocortisolism.
Now, a paper by Peter Kühnen and colleagues published in the New England Journal of Medicine, shows that treating patients with the melanocortin-4 receptor agonist, setmelanotide, can result in significant reduction in appetite and body weight.
The open-label study was performed in two adult patients with POMC deficiency, in cooperation with Rhythm Pharmaceuticals, which provided the study medication and regulatory support.
Both patients weighed around 150 Kg with marked hyperphagia and both responded to treatment with a substantial reduction in appetite and dramatic weight loss of over 20 Kg over 12-13 weeks.
After a brief interruption, one patient was again treated for 42 weeks, ultimately losing 51 kg (32.9% of her initial body weight).
As the authors note,
“Setmelanotide appeared to completely reverse hyperphagia, leading to impressive weight loss and normalization of insulin resistance. More important, both patients reported a dramatic improvement in their quality of life after the initiation of setmelanotide therapy. Moreover, the substantial and ongoing reduction in body weight was similar to the changes observed after leptin administration in patients with leptin deficiency.”
Over all the treatment was well tolerated with no major adverse effects.
While these observations were made in very rare patients with documented POMC deficiency, these findings may have broader implications for individuals with more common “garden-variety” obesity.
“Both patients described here had very high leptin levels before treatment, suggesting leptin resistance. In patients with proopiomelanocortin deficiency, the leptin signal is probably not properly transduced into anorexigenic responses, given the lack of melanocyte-stimulating hormone. Setmelanotide substitutes for melanocyte-stimulating hormone and binds at its receptor, thus overcoming leptin resistance. On the basis of the observation that obese patients without known genetic abnormalities have severe leptin resistance and regain weight owing to a post-dieting increase in appetite, we speculate that setmelanotide may also be effective in nongenetic forms of obesity.”
Appropriate studies in patients with non-POMC deficient obesity are currently underway.
@DrSharma
Atlanta, GA
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
