The Vast Majority Of Healthy Women Will Become Unhealthy!
 Most healthy women, who live long enough, will eventually become unhealthy.
Most healthy women, who live long enough, will eventually become unhealthy.
So it should not at all come as a surprise to anyone, that the vast majority of women with “healthy” obesity (a misnomer, as in my view, the medical term “obesity” should only apply to people who already have health problems attributable to abnormal or excess body fat), eventually end up with “unhealthy” obesity.
This, essentially, is the gist of a paper by Nathalie Eckel and colleagues, published in The Lancet.
In their study of 90,257 participants of the Nurses Health Study, who were followed-up from 1980 to 2010 for incident cardiovascular disease (representing over 2 million person-years of follow-up), they found that around 80% of metabolically healthy women with obesity converted to metabolically unhealthy obesity over the course of follow-up.
But one might say that this was only marginally higher that the 70% of metabolically healthy “normal weight” women, who also converted to metabolically unhealthy over the 20 years of observation. In fact, the population-attributable risk of the latter group was much higher, as it consisted of almost 10 times the number of women than in the former.
While the risk of cardiovascular disease was statistically elevated (by about 40%) in the metabolically healthy women with obesity, this risk was 243% higher in metabolically unhealthy women with normal weight, 260% higher in metabolically unhealthy women with overweight and 315% higher in metabolically unhealthy women with obesity, all compared to metabolically healthy women with normal weight.
So, yes, women with metabolically “healthy obesity” have a high risk of becoming metabolically unhealty and developing cardiovascular disease, so are metabolically healthy normal-weight women.
Overall, I believe it is safe to say that the vast majority of metabolically healthy women (regardless of body weight) will eventually become metabolically unhealthy, at which time their risk for cardiovascular disease increases.
Bottom line, everyone (not just women with obesity) will benefit from efforts to stay as metabolically healthy as possible for as long as possible – fortunately, we know that healthy diets and regular physical activity (while not necessarily preventing weight gain) can help maintain metabolic health, irrespective of current body weight.
Clearly, living as healthy as possible is not just good advice for women with obesity – who would have guessed?
@DrSharma
Edmonton, AB
p.s. although this was a study in women, I have no doubt whatsoever that the findings also apply to men – most metabolically healthy men will eventually become metabolically unhealthy over the course of their lifetime.
The Heterogeneity of Obesity
 In the same manner in that there is not one predisposing factor for the development of obesity, the phenotypic clinical presentation of obesity is likewise extraordinarily heterogenous. (This has some authors speaking of “obesities” rather than “obesity”).
In the same manner in that there is not one predisposing factor for the development of obesity, the phenotypic clinical presentation of obesity is likewise extraordinarily heterogenous. (This has some authors speaking of “obesities” rather than “obesity”).
While it is now well established that BMI is a measure of size rather than health, it is perhaps less well recognised how the different types of body fat and their storage in various fat depots and organs can contribute to cardiometabolic disease (location, location, location!).
Now, a comprehensive review by Ian Neeland from the University of Texas Southwestern Medical Center, Dallas, together with my colleagues Paul Poirier and JP Despres from Laval University in Quebec, published in Circulation discusses the cardiovascular and metabolic heterogeneity of obesity.
As the authors point out,
“Although the BMI has been a convenient and simple index to monitor the growth in obesity prevalence at the population level, many metabolic and clinical studies have revealed that obesity, when defined on the basis of the BMI alone, is a remarkably heterogeneous condition. For instance, patients with similar body weight or BMI values have been shown to display markedly different comorbidities and levels of health risk.”
Not only has BMI never emerged as a significant component in risk engines such as the Framingham risk score, there are many individuals with obesity who never develop metabolic complications or heart disease during the course of their life.
The paper offers a good review of what the author describe as adipose dysfunction or “adiposopathy” = “sick fat”. Thus, in some individuals, there is an accumulation of “unhealthy” fat (particularly visceral and ectopic fat), whereas in others, excess fat predominantly consists of “healthy” fat (predominantly in subcutaneous depots such as the hips and thighs).
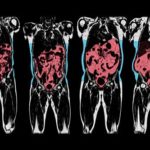
The authors thus emphasise the importance of measuring fat location with methods ranging from simple anthropometric measures (e.g. waist circumference) to comprehensive imaging techniques (e.g. MRI).
The authors also provide a succinct overview of exactly how this “sick fat” contributes to cardiometabolic risk and briefly touches on the behavioural, medical, and surgical management of patients with obesity and elevated cardiometabolic risk.
I, for one, was also happy to see the inclusion of the Edmonton Obesity Staging System in their reflections on this complex issue.
This paper is certainly suggested reading for anyone interested in the link between obesity and cardiovascular disease.
@DrSharma
Edmonton, AB
Fit-Fat Paradox Holds For People With Severe Obesity
 Regular readers will be quite familiar with the findings that cardiometabolic health appears to be far more related to “fitness” than to “fatness” – in other words, it is quite possible to mitigate the metabolic risks commonly associated with excess body fat by improving cardiorespiratory fitness.
Regular readers will be quite familiar with the findings that cardiometabolic health appears to be far more related to “fitness” than to “fatness” – in other words, it is quite possible to mitigate the metabolic risks commonly associated with excess body fat by improving cardiorespiratory fitness.
Now, a study by Kathy Do and colleagues from York University, Toronto, published in BMC Obesity, shows that this relationship also holds for people with quite severe obesity.
The researcher studied 853 patients from the Wharton Medical Clinics in the Greater Toronto Area, who completed a clinical examination and maximal treadmill test. Patients were then categorized into fit and unfit based on age- and sex-categories and in terms of fatness based on BMI class.
Within the sample, 41% of participants with mild obesity (BMI<35) had high fitness whereas only 25% and 11% of the participants with moderate (BMI 35-40) and severe obesity (BMI>40), respectively, had high fitness.
Individuals with higher fitness tended to be younger and more likely to be female.
While overall fitness did not appear to be independently associated with most of the metabolic risk factors (except systolic blood pressure and triglycerides), the effect of fitness in patients with severe obesity was more pronounced. Thus, the prevalent relative risk for pre-clinical hypertension, hypertriglyceridemia and hypoalphalipoproteinemia and pre-diabetes was only elevated in the unfit moderate and severe obesity groups, and fitness groups were only significantly different in their relative risk for prevalent pre-clinical hypertension within the severe obesity group.
Similarly, high fitness was associated with smaller waist circumferences, with differences between high and low fitness being larger in those with severe obesity than with mild obesity.
Based on these findings, the researchers conclude that the favourable associations of having high fitness on health may be similar if not augmented in individuals with severe compared to mild obesity.
However, it is also apparent based on the rather low number of “fit” individuals in the severe obesity category (only about 1 in 10), that maintaining a high level of fitness proves to be more challenging the higher the BMI.
@DrSharma
Edmonton, AB
Can Liraglutide Help Grow New Fat Cells?
 The human GLP-1 analogue liraglutide is now approved for the long-term medical treatment of obesity in an ever-increasing number of countries. Its safety and clinical effectiveness is now well established and there is no doubt that this is an important addition to the rather limited number of treatment options available to people living with obesity.
The human GLP-1 analogue liraglutide is now approved for the long-term medical treatment of obesity in an ever-increasing number of countries. Its safety and clinical effectiveness is now well established and there is no doubt that this is an important addition to the rather limited number of treatment options available to people living with obesity.
Interestingly, however, liraglutide has also been shown to promote the differentiation of pre-adipocytes or, in other words, promote the formation of new fat cells.
While this may seen worrying or even counter-intuitive, we much remember that having more (smaller) rather than fewer (bigger) fat cells actually has substantial metabolic advantage s- there is indeed ample data showing that large adipocyte cell size and limited capacity to grow fat cells (the extreme case of which is seen in people with lipodystrophy) is actually a key risk factor for metabolic problems including insulin resistance, possible by promoting the accumulation of ectopic fat (e.g. in liver and skeletal muscle).
Now, a paper by Yongmei Liand colleagues, published in Molecular Medicine Reports provides additional insight into the cellular pathways involved in liraglutide’s adipogenic effects.
Using a series of in vitro experiments, the researchers show that liraglutide does indeed promote the adipogenic differentiation of 3T3-L1 cells (a widely used murine preadipocyte cell line) through a process that upregulates the expression of C/EBPα and PPARγ at the early phase of adipogenic differentiation, promots the expression of lipogenesis associated genes including aP2, and enhances the accumulated of lipids.
At the same time, liraglutide appears to suppress cell proliferation via the Hippo‑yes‑associated protein (YAP) signaling pathway, thereby allowing these cells to transform into mature adipocytes sooner.
How relevant these observations are for humans remains to be seen, but certainly the promotion of adipogenic differentiation may hold the potential for improving insulin sensitivity and reducing the metabolic risks associated with excess weight gain.
@DrSharma
Edmonton, AB
Disclaimer: I have received speaking and consulting honoraria from Novo Nordisk, the maker of liraglutide.
Reducing Cardiovascular Risk In Adolescents With Bariatric Surgery
 Given the limited effectiveness of “lifestyle” interventions and the lack of access to medical treatments, many adolescents struggling with severe obesity are left with no option but to consider having bariatric surgery.
Given the limited effectiveness of “lifestyle” interventions and the lack of access to medical treatments, many adolescents struggling with severe obesity are left with no option but to consider having bariatric surgery.
Now, a paper by Marc Michalsky and colleagues on behalf of the Teens LABS Consortium, in a paper published in Pediatrics, describes the effect of bariatric surgery on cardiovascular risk factors in adolescents undergoing these procedures.
The study includes 242 adolescents (76% girls, 72% white, mean age 17 ± 1.6 y, median BMI 51) undergoing bariatric surgery (Roux-en-Y gastric bypass (n = 161), vertical sleeve gastrectomy (n = 67), or adjustable gastric banding (n = 14)), at five centers.
At 3 years following surgery, weight was significantly lower in all groups (28%, 26%, and 8% for RYGB, VSG, and AGB, respectively).
Hypertension, observed in 44% of participants, declined to 15% at 3 years.
Dyslipidemia observed in 75% of participants, declining to 27% by 1 year and 29% by 3 years. This improvement was largely due to decrease in triclycerides and increases in HDL cholesterol.
Baseline diabetes was present in 13% of participants with major metabolic improvement (0.5%) by 3 years. Similarly, baseline impaired fasting glucose (26%) and hyperinsulinemia (74%) dramatically improved by year 3 (4% and 20%, respectively).
Improvements in these parameters were related to the degree of weight loss.
Remission rates were negatively correlated to higher age and positively correlated to female sex and white race.
Overall, the authors conclude that this study documents the improvements in cardiovascular risk factors in adolescent bariatric surgery.
Unfortunately, the study does not present any information on surgical complications or reoperation rates, an obvious matter of concern when it comes to surgery in this young population.
While there may well have been no alternative to surgical treatment in these kids, we can only hope that eventually medical treatments will become available for this population, hopefully with similar outcomes. Unfortunately, that may well still be a long way off.
@DrSharma
Edmonton, AB
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
