No One Should Be Surprised That There Are Skinny Genes
 Anyone who has ever seriously looked at the genetics of obesity should be well aware that body weight and size is a highly heritable trait.
Anyone who has ever seriously looked at the genetics of obesity should be well aware that body weight and size is a highly heritable trait.
As one may expect, this heritability extends across the entire spectrum of body size. Thus, if there are genes that explain obesity, then perhaps certain variations of these very same genes may do the exact opposite – i.e. promote “skinniness”.
In fact, we all know these people, who appear to be highly weight-gain “resistant”, in that they can apparently eat all day without gaining a gram of body fat or simply find it very difficult to “overeat” even when surrounded by highly-palatable food.
Now, a study by Fernando Riveros-McKay and colleagues, published in PLOS Genetics, compares the genetics of thinness with that of severe obesity.
Using genome-wide association studies, the researchers not only show that the heritability of thinness was comparable to that of severe obesity but they also confirmed the existence of 10 genetic loci that had been previously associated with obesity (as well as an addition obesity and BMI-associated locus (PKHD1).
As there may well be non-genetic reasons for people to fall into the “thin” end of the size spectrum, the researchers were careful to only include individuals who appeared in good health and especially excluded individuals with anorexia.
Overall, these finding are consistent with animal studies that have also identified loci/genes associated with thinness/decreased body weight due to reduced food intake/increased energy expenditure/resistance to high fat diet-induced obesity, mechanisms that the authors hypothesise may also contribute to human thinness.
Clearly, further genetic and phenotypic studies focused on persistently thin individuals may provide new insights into the mechanisms regulating human energy balance and may uncover potential anti-obesity drug targets.
@DrSharma
Edmonton, AB
Factors Affecting Energy Metabolism: Genetics, Sex, and Aging
Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect metabolic rate:
Genetics
Because heritable factors appear to be responsible for 45–75% of the inter‐individual variation in body mass index (BMI), the potential impact of genetic determinants of metabolic rate upon the predisposition to obesity must be considered. While numerous somatic and mitochondrial genes with potential effects on metabolic rate have been identified, their contribution to human obesity has yet to be defined Likewise, although there is preliminary evidence for intrauterine and perinatal programming of genes involved in energy metabolism, their role in human obesity remain unclear. What is apparent is that the genetic predisposition to obesity (including both energy intake and metabolism) is not explainable on the basis of a small number of common mutations exerting substantial effects on the individual tendency to weight gain. Thus, a great deal of work is still required before investigation into the multitude of genetic determinants of body weight can potentially impact clinical management. Currently, a careful clinical assessment of family history of obesity and related risk factors remains the best measure of genetic risk for obesity.
Sex
There is a clear effect of gender [sic] on metabolic requirements, whereby, for the same BMI, women consistently display lower metabolic rates (approximately 20% less) than men, largely accounted for by differences in fat‐free mass (FFM).
Aging
Aging is an important determinant of a decline in metabolic rate, with an estimated reduction of around 150 kcal per decade of adult life. Factors that result in the age‐related decline in energy requirements include changes in neuroendocrine factors (e.g. sympathetic activity, thyroid function, etc.) as well as a reduction in skeletal muscle quantity and quality (resulting from reduced physical activity, reduced protein intake and other less‐well‐understood factors).
Additional factors that can affect metabolic rate will be discussed in subsequent posts.
@DrSharma
Edmonton, AB
Molecular Changes During Weight Gain – Everyone Is Different
 As one may well imagine, changes in body weight (up or down) can profoundly affect a vast number of hormonal and metabolic pathways.
As one may well imagine, changes in body weight (up or down) can profoundly affect a vast number of hormonal and metabolic pathways.
Now, a team of researchers led by Brian Piening and colleagues, in a paper published in Cell Systems used a broad “omics” based approach to study what happens when people lose ore gain weight.
Specifically, the goal of this study was to:
(1) assemble a comprehensive map of the molecular changes in humans (in circulating blood as well as the microbiome) that occur over the course of a carefully controlled weight gain and their reversibility with weight loss; and
(2) determine whether inulin sensitive (IS) and insulin resistant (IR) individuals who are matched for degree of obesity demonstrate unique biomolecular signatures and/or pathway activation during similar weight gain.
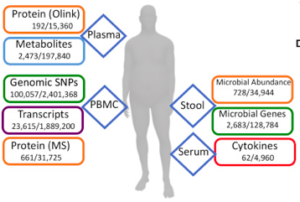
The study included 23 carefully selected healthy participants with BMI 25–35 kg/m2, were studied. Samples were collected at baseline. They then underwent a 30-day weight gain period (average 2.8 kg), followed by an eucaloric diet for 7 days, at which point a second fasted sample of blood and stool was collected. Each participant then underwent a caloric-restricted diet under nutritionist supervision for a subsequent 60-day period designed to return each participant back to his/her initial baseline weight, at which point a third set of fasted samples of blood and stool were collected. A subset of participants returned for a follow-up sampling approximately 3 months after the end of the perturbation.Insulin resistance was assessed at baseline using a modified insulin suppression test.
The large-scale multi-omics assays performed at all time points on each participant included genomics, proteomics, metabolomics and microbiomics.
Despite some differences between the IS and IR group (particularly in differential regulation of inflammatory/immune response pathways), overall, molecular changes were dominated by inter-personal variation (i.e. changes within the same individual), which accounted for more than 90% of the observed variance in some cases (e.g., cytokines). The most striking changes with weight gain were in inflammation response pathways (despite the rather modest weight gain) and were (fortunately) reversed by weight loss.
As the authors note,
“Comparing the variation in cytokine levels between multiple baselines in a single individual versus across individuals, we observed a striking difference: for almost all cytokines, the within-individual coefficient of variation was under 20%, whereas the variation across individuals was 40%–60%. This shows that our baseline cytokine profiles are unique to the individual, a point that has significant implications for one-size-fits-all clinical cytokine assays for the detection and/or monitoring of disease.”
On the opposite side of the spectrum, proteomics and metabolomics measurements had a substantial unexplained component (30% and 35%, respectively), highlighting the presence of unaccounted factors (e.g., food, exercise, and other changing environmental factors) or a subject-specific reaction to the perturbation.
Notably, not all of the responses we observed were consistent across IR and IS participants.
“In particular, for the microbiome, we observed that the microbe A. muciniphila was weight gain responsive only in insulin-sensitive participants. The abundance of this particular microbe in IR individuals did not change across perturbations and was barely or not detectable in most IR individuals.”
Clearly, these findings highlight the fact that each individual is biochemically unique, which the authors note, makes a strong case for personalized analysis in medicine.
Perhaps more importantly for researchers, nearly all of the data are publicly available, enabling exploration of inter-omic relationships and alterations across a longitudinal perturbation, thus providing a valuable resource for the development and validation of bioinformatic tools and pipelines integrating disparate data types.
@DrSharms
Edmonton, AB
How Precise Can Obesity Medicine Get?
 Another article in the 2018 JAMA special issue on obesity is one by Susan and Jack Yanovski and deals with the issue of using a precision or “personalised” approach to obesity prevention and management.
Another article in the 2018 JAMA special issue on obesity is one by Susan and Jack Yanovski and deals with the issue of using a precision or “personalised” approach to obesity prevention and management.
As we know, there are myriad factors that can lead to obesity (environmental, genetic, psychological, medical, etc., etc., etc.), with each patient having their own story and set of drivers and barriers.
Furthermore, we know that for any given treatment (whether behavioural, medical, or surgical) there is wide variation in individual outcomes.
So, being able to match the right treatment to the right patient, or even better, reliably predict a given patient’s response to a specific treatment could potentially improve outcomes and reduce patient burden and costs.
However, as the authors note, currently the only real predictor to treatment response is how well patients respond during the early part of treatment. Thus, we know that patient who lose a significant amount of weight during the first few weeks of medical treatment, tend to have the best long-term success in terms of weight loss.
However, this approach is also rather limited. In my own practice, I regularly see patients, who initially do well with behavioural, medical or surgical treatments, but eventually struggle, as well as patients who take longer to respond to a treatment before ultimately doing fine in the long term.
We are of course a long way off from having any kind of genetic or other testing that would reliably predict patient responses to treatment.
While this may become possible in the future, I am not holding my breath.
Not only is every patient’s story different, but the many factors that can determine response (societal, behavioural, psychological, biological, etc.) are almost endless and, moreover, can even vary over time in a given individual.
In fact, for most complex chronic diseases (e.g. diabetes, hypertension, depression, etc.), finding the best treatment for a given patient continues to be “trial and error”, or in other words, “empirical”.
Despite all the progress in genetic research, this has not really changed for most other complex chronic diseases like hypertension, type 2 diabetes, or dyslipidemia (despite a few rare but notable exceptions).
Moveover, as the authors point out, there are many other factors that will determine whether or not a given patient even has access to certain treatments, irrespective of whether or not that treatment is indeed the best treatment for them.
Currently, the best we can do, is to try to understand the drivers and barriers that each of our patients face and discuss with them the best treatment options available to them given their situation and circumstances.
Whether a more precise approach is ever likely (as the authors hope), clearly remains to be seen, but based on the progress made in for other complex chronic conditions, for which similar approaches have been tried, I am perhaps far less optimistic than the authors.
But, then again, I am happy to be proven wrong.
@DrSharma
Edmonton, AB
The Key To Obesity Management Lies In The Science Of Energy Homeostasis
 If there is one thing we know for sure about obesity management, it is the sad fact, that no diet, exercise, medication, not even bariatric surgery, will permanently reset the body’s tendency to defend and regain its body weight to its set point – this generally being the highest weight that has been achieved and maintained for a notable length of time.
If there is one thing we know for sure about obesity management, it is the sad fact, that no diet, exercise, medication, not even bariatric surgery, will permanently reset the body’s tendency to defend and regain its body weight to its set point – this generally being the highest weight that has been achieved and maintained for a notable length of time.
Thus, any effective long-term treatment has to offset the complex neurobiology that will eventually doom every weight-loss attempt to “failure” (no, anecdotes don’t count!).
Just how complex and overpowering this biological system that regulates body weight is, is described in a comprehensive review by the undisputed leaders in this field (Michael Schwartz, Randy Seeley, Eric Ravussin, Rudolph Leibel and colleagues) published in Endocrine Reviews. Indeed the paper is nothing less than a “Scientific Statement” from the venerable Endocrine Society, or, in other words, these folks know what they’re talking about when it comes to the science of energy balance.
As the authors remind us,
“In its third year of existence, the Endocrine Society elected Sir Harvey Cushing as President. In his presidential address, he advocated strongly in favor of adopting the scientific method and abandoning empiricism to better inform the diagnosis and treatment of endocrine disease. In doing so, Cushing helped to usher in the modern era of endocrinology and with it, the end of organo-therapy. (In an interesting historical footnote, Cushing’s Energy Homeostasis and the Physiological Control of Body-Fat Stores presidential address was given in , the same year that insulin was discovered.)”
Over 30 pages, backed by almost 350 scientific citations, the authors outline in excruciating detail just how complex the biological system that regulates, defends, and restores body weight actually is. Moreover, this system is not static but rather, is strongly influenced and modulated by environmental and societal factors.
Indeed, after reading this article, it seems that the very notion, that average Jane or Joe could somehow learn to permanently overcome this intricately fine-tuned system (or the societal drivers) with will power alone is almost laughable (hats off to the very few brave and determined individuals, who can actually do this – you have climbed to the top of Mount Everest and decided to camp out there for the foreseeable future – I wish you all the best!).
Thus, the authors are confident that,
“The identification of neuromolecular mechanisms that integrate short-term and long-term control of feeding behavior, such that calorie intake precisely matches energy expenditure over long time intervals, will almost certainly enable better preventive and therapeutic approaches to obesity.”
Sadly, despite all we have learnt about this system, we are still far from fully understanding it. Thus, the canonical molecular/ cellular signaling pathway: LEP → LEPR → POMC, AgRP → PC → MC4R is just one pathway in a complex network of multiple interacting and sometimes redundant pathways that involve virtually every part of the brain.
Also, the effect of environmental factors appears to be far more complex than most people think. Thus,
“During sensitive periods of development, ontogenic processes in both brain and peripheral organs can be modified so as to match anticipated environmental conditions. Although many exposures during development could potentially predispose to obesity in adulthood, we focus here on two that some researchers think contribute to the secular trends in obesity: parental obesity and exposure to endocrine disrupting chemicals (EDCs).”
Throw in the role of gut bugs, infections, and societal factors, and it is easy to see why no simple solution to the obesity epidemic are in sight (let alone a range of effective long-term treatments like we have for most other common chronic diseases).
As for solutions,
“To be viable, theories of obesity pathogenesis must account not only for how excess body fat is acquired, but also for how excess body fat comes to be biologically defended. To date, the preponderance of research has focused on the former. However, we must consider the possibility that some (perhaps even most) mechanisms underlying weight gain are distinct from those responsible for the biological defense of excess fat mass. A key question, therefore, is how the energy homeostasis system comes to defend an elevated level of fat mass (analogous to the defense of elevated blood pressure in patients with hypertension). Answering this question requires an improved understanding of the neuro-molecular elements that underlie a “defended” level of body fat. What are the molecular/neuroanatomic predicates that help establish and defend a “set point” for adiposity? How do these elements regulate feeding behavior and/or energy expenditure, so as to achieve long-term energy balance? By what mechanisms is an apparently higher set point established and defended in individuals who are obese?” [sic]
Clearly,
“Given that recovery of lost weight (the normal, physiological response to weight loss irrespective of one’s starting weight) is the largest single obstacle to effective long-term weight loss, we cannot overstate the importance of a coherent understanding of obesity-associated alterations of the energy homeostasis system.”
There is much work to be done. Whether or not, in this climate of anti- and pseudo-science, funding for such fundamental work will actually be made available, is anyone’s guess.
@DrSharma
Edmonton, AB
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
