Time To Change The Obesity Narrative
 This week, I once again presented on the need for recognising obesity as a chronic disease at the annual European Society for the Study of Obesity Collaborating Centres for Obesity (EASO-COMs) in Leipzig, Germany.
This week, I once again presented on the need for recognising obesity as a chronic disease at the annual European Society for the Study of Obesity Collaborating Centres for Obesity (EASO-COMs) in Leipzig, Germany.
Coincidently, The Lancet this week also published a commentary (of which I am a co-author) on the urgent need to change the obesity “narrative”.
So far, the prevailing obesity “narrative” is that this is a condition largely caused by people’s lifestyle “choices” primarily pertaining to eating too much and not moving enough, and that this condition can therefore be prevented and reversed simply by getting people to make better choices, or in other words, eating less and moving more.
As pointed out in the commentary, this “narrative” flies in the face of the overwhelming evidence that obesity is a rather complex multi-factorial heterogenous disorder, where long-term success of individual or population-based “lifestyle” interventions can be characterised as rather modest (and that is being rather generous).
This is not to say that public health measures targeting food intake and activity are not important – but these measures go well beyond “personal responsibility”
” The established narrative on obesity relies on a simplistic causal model with language that generally places blame on individuals who bear sole responsibility for their obesity. This approach disregards the complex interplay between factors not within individuals’ control (eg, epigenetic, biological, psychosocial) and powerful wider environmental factors and activity by industry (eg, food availability and price, the built environment, manufacturers’ marketing, policies, culture) that underpin obesity. A siloed focus on individual responsibility leads to a failure to address these wider factors for which government policy can and should take a leading role. Potential health-systems solutions are also held back by insufficient understanding of obesity as a chronic disease and of the necessary integration across specialties.“
It is also important to recognise that the prevailing “lifestyle” narrative plays a major role in the issue of weight-bias and discrimination:
“Behind every obesity statistic are real people living with obesity. The prevailing narrative wrongly portrays people with obesity in negative terms as “guilty” of obesity through “weakness” and “lack of willpower”, succumbing to the siren call of fast and other poor food choices. This narrative leads to stigmatisation, discrimination—including in health services, employment, and education—and undermines individual agency.“
Thus, it is time to change this narrative:
“If the narrative is instead reframed around individuals at risk of or living with obesity as protagonists with agency who operate within physiological limitations and a much larger obesogenic environment over which their control is limited, then a better, more accurate story can be told.“
This new narrative must incorporate four dimensions.
“First, recognise that obesity requires multiple discrete actors and sectors to work together simultaneously through many entry points. Second, change the words and images used to portray obesity to shift blame away from individuals and towards upstream drivers. For example, photographs of anonymous or faceless people with obesity must be substituted with images of real people that foster respect and identification. Third, prioritise childhood obesity and the growing burden of obesity in low-income settings. Rights-based policy approaches that address inequalities and social and physical determinants of obesity are particularly relevant. Finally, appreciate that obesity is a chronic disease within the health system, with both its prevention and management embedded within calls for effective and comprehensive universal health coverage globally.“
Following this line of reasoning we argue that,
“Shifting to a human-focused narrative that encompasses this vulnerability and complexity will require effort and commitment across many sectors. We call on all affected by or concerned with obesity to come together with a common sense of purpose and shared accountability for building this new narrative and a more comprehensive response to obesity.“
Not discussed in this paper (largely due to space limitation), is my pet peeve, that we also need a new non-anthropometric definition of obesity – one that relies on actual health measures rather than just scales and measuring tapes. As we move to a “disease” definition of obesity, we need to ensure that we are not mis-labeling healthy individuals as “diseased” just because they happen to exceed a certain body weight, as well as the corollary, mis-labeling individuals who may stand to benefit from obesity treatments as not having obesity just because they fall below an arbitrary BMI cutoff.
@DrSharma
Leipzig, Germany
Some Limitations In Applying The Etiological Framework To Obesity Assessment
 To conclude this series of citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, that guides us through a systematic assessment of factors influencing energy metabolism, ingestive behaviour, and physical activity, it is important to consider some limitations of this (and any other) etiological approach to obesity management:
To conclude this series of citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, that guides us through a systematic assessment of factors influencing energy metabolism, ingestive behaviour, and physical activity, it is important to consider some limitations of this (and any other) etiological approach to obesity management:
While we have taken efforts to provide a comprehensive and wide‐ranging list of considerations in the assessment of obesity, we fully recognize that a full work‐up of all permutations of the proposed factors may well be beyond the scope of a busy practitioner. In this regard, the old saying applies: ‘when you hear hoofs, think of horses not zebras’. Thus, consideration should be first given to the most common and obvious reasons laid out in this paper, many of which should be immediately apparent to the experienced clinician (e.g. homeostatic hyperphagia resulting from meal skipping, hedonic hyperphagia related to depression, immobility due to osteoarthritis, weight gain due to atypical antipsychotics, etc.). Also, the use of comprehensive self‐directed questionnaires such as the Weight and Lifestyle Inventory, a multiple‐page self‐report questionnaire that the patient completes before treatment visits, designed to identify the root causes of obesity and perform an environmental analysis, may be helpful in this regard. Future efforts must also aim to provide simple clinical algorithms that will guide the busy clinician through the maze of factors that can potentially precipitate and/or exacerbate positive energy balance.
Nevertheless, as in a patient with oedema, despite complete recognition of the underlying factors, the clinician often has no option but to manage the patient with the judicious use of fluid restriction and diuretics. Similarly, in patients presenting with obesity, the underlying contributing factors (e.g. genetics, addiction, depression, back pain, etc.) may not be easily amenable to causal treatment. In these cases, ‘symptomatic’ treatment of obesity with caloric restriction and exercise regimens may well in many cases prove to be the only option. Nevertheless, we maintain that careful identification and management of the possible socio‐cultural, psychological and biomedical barriers will likely increase the feasibility, compliance and adherence to these measures. Recognition of the causes and barriers will also help set out realistic expectations regarding the degree of weight loss that is likely to be achievable and sustainable, an important aspect of weight management. Despite the increased time required for the comprehensive work‐up of an obese patient, we believe that this framework will eventually save costs by allowing clinicians to specifically identify and target the causes and barriers of positive energy balance, rather than resorting to the ‘one‐size‐fits‐all’ (eat less – move more) approach to obesity, which given its limited efficacy, can only be considered wasteful.
Commentary: While the proposed etiological framework can help understand why a given person may have obesity, and, more importantly, help identify important barriers to weight management, we must also realise that virtually every patient, irrespective of the underlying drivers or weight gain will face the same biological challenges when it comes to long-term weight loss – the fact remains, that our bodies can harness a host of powerful neuroendocrine mechanisms to defend against weight loss and promote weight regain. This is why in clinical practice, I often see that the best that addressing the underlying cause of weight gain achieves is the slowing or elimination of further weight gain. Thus, for example, even if painful arthritis and immobility may have caused weight gain in a given patient, a joint replacement will not automatically result in weight loss. Similarly, taking a patient of an atypical anti-pyschotic will not lead to much weight loss, nor will treatment of sleep apnea. When you remove the cause of weight gain – you stop weight gain – you do not generally reverse the process and end up with significant persistent weight loss. Thus, identifying and addressing the drivers of weight gain is only the first step in obesity management. Once weight is stabilized, we can proceed with developing a treatment plan for sustainable weight loss (as indicated).
@DrSharma
Edmonton, AB
Factors Affecting Ingestive Behaviour: Physiological or Homeostatic Factors
 Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour:
Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour:
Physiological or Homeostatic Factors
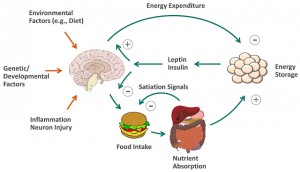
In contrast to excess caloric consumption that results largely from environmental determinants, over‐eating in response to increased hunger or reduced satiety can be viewed as a physiological response to a perturbation of the homeostatic system and is perhaps best termed homeostatic hyperphagia. Primary homeostatic hyperphagia can result from genetic defects in the homeostatic system (e.g. leptin deficiency, melanocortin type 4 receptor mutation or Prader Willi Syndrome) and are rare. Secondary homeostatic hyperphagia can result from acquired defects or perturbations in the homeostatic system (e.g. head trauma, craniopharyngeoma, insulinoma). Tertiary homeostatic hyperphagia, by far the most common category, is largely the result of inappropriate feeding intervals and/or nutrient selection. Thus, skipping meals, resulting in a compensatory hyperphagic response (rapid ingestion of energy‐dense foods), is perhaps the most prevalent form of homeostatic hyperphagia. Ingestion of high‐glycemic foods resulting in a rapid rise and fall in blood glucose and insulin levels (‘crash and crave’) may prompt increased snacking and overconsumption, although this notion remains controversial. Meal duration and composition can also affect satiety response, whereby delayed or reduced satiation (e.g. in response to hasty eating, energy‐dense foods, low fibre intake, liquid calories) can result in excess caloric intake. The presence of homeostatic hyperphagia (characterized by over‐eating in response to increased hunger and/or reduced satiety) will likely call for interventions that specifically address the underlying perturbation in this system (e.g. administration of leptin, excision of the insulinoma, correction of meal pattern, nutritional hygiene, portion control, etc.). Patients with obesity resulting from tertiary homeostatic hyperphagia are the most likely to benefit from dietary counselling.
@DrSharma
Edmonton, AB
The Canadian Obesity Network Is No More – Long Live Obesity Canada!
 Over a decade ago, together with over 120 colleagues from across Canada, representing over 30 Canadian Universities and Institutions, I helped found the Canadian Obesity Network with the support of funding from the Canadian National Centres of Excellence Program.
Over a decade ago, together with over 120 colleagues from across Canada, representing over 30 Canadian Universities and Institutions, I helped found the Canadian Obesity Network with the support of funding from the Canadian National Centres of Excellence Program.
Since then the Canadian Obesity Network has grown into a large and influential organisation, with well over 20,000 professional members and public supporters, with a significant range across Canada and beyond.
During the course of its existence, the Network has organised countless educational events for health professionals, provided training and networking opportunities to a host of young researchers and trainees, developed a suite of obesity management tools (e.g. the 5As of obesity management for adults, kids and during pregnancy), held National Obesity Summits and National Student Meetings. raised funds for obesity research, the list of achievements goes on and on.
Most importantly, the Network has taken on important new roles in public engagement, voicing the needs and concerns of Canadians living with obesity, and advocating for better access to evidence-based prevention and treatments for children and adults across Canada.
To better reflect this expanded mission and vision, the Board of Directors has decided to convert the Canadian Obesity Network into a registered health charity under the new name – Obesity Canada – Obésité Canada.
So with one sad eye, I look back and hope that the Canadian Obesity Network rests in peace – Long Live Obesity Canada!
@DrSharma
Edmonton, AB
Etiological Assessment of Obesity: Factors Affecting Ingestive Behaviour
 Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour. Once you have quickly established that weight gain is not primarily driven by a change (decrease) in metabolic requirements, you turn to the most likely cause of weight gain – eating more calories than your body actually needs:
Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour. Once you have quickly established that weight gain is not primarily driven by a change (decrease) in metabolic requirements, you turn to the most likely cause of weight gain – eating more calories than your body actually needs:
Ingestive behaviour, which includes both eating and drinking, accounts for 100% of total energy intake. In contrast to total energy expenditure, caloric intake (on a daily basis) can vary from zero (fasting) to several times that of total energy requirements (e.g. during a binge eating episode). Given the ease with which it is possible for energy intake to exceed caloric expenditure, it is therefore not surprising that caloric hyperalimentation is a major determinant of weight gain. Any assessment of obesity or increase in body weight thus requires a careful assessment of ingestive behaviour. Evidence for caloric hyperalimentation or hyperphagia should in turn prompt systematic exploration of the determinants of this behaviour. In this context, it helps to view over‐eating as a symptom of an underlying perturbation of ingestive behaviour rather than simply a wilful behavioural choice.
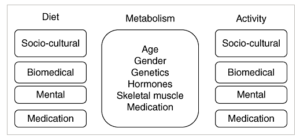
While the socio‐psycho‐neurobiological determinants of ingestive behaviour are exceedingly complex, in clinical practice, it is possible to divide them into four domains: socio‐cultural factors, biomedical or physiological (homeostatic) factors, psychological (hedonic) factors and medications. In a given individual, these domains are intimately connected and show considerable variation and overlap. Nevertheless, in practice it is often possible to determine the primary domain that explains the excess caloric intake in a given individual and can thus provide the key to developing a treatment plan that addresses the root cause of this behaviour.
More on the various factors affecting ingestive behaviour in coming posts.
@DrSharma
Edmonton, AB
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
