Can Liraglutide Help Grow New Fat Cells?
 The human GLP-1 analogue liraglutide is now approved for the long-term medical treatment of obesity in an ever-increasing number of countries. Its safety and clinical effectiveness is now well established and there is no doubt that this is an important addition to the rather limited number of treatment options available to people living with obesity.
The human GLP-1 analogue liraglutide is now approved for the long-term medical treatment of obesity in an ever-increasing number of countries. Its safety and clinical effectiveness is now well established and there is no doubt that this is an important addition to the rather limited number of treatment options available to people living with obesity.
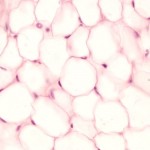
Interestingly, however, liraglutide has also been shown to promote the differentiation of pre-adipocytes or, in other words, promote the formation of new fat cells.
While this may seen worrying or even counter-intuitive, we much remember that having more (smaller) rather than fewer (bigger) fat cells actually has substantial metabolic advantage s- there is indeed ample data showing that large adipocyte cell size and limited capacity to grow fat cells (the extreme case of which is seen in people with lipodystrophy) is actually a key risk factor for metabolic problems including insulin resistance, possible by promoting the accumulation of ectopic fat (e.g. in liver and skeletal muscle).
Now, a paper by Yongmei Liand colleagues, published in Molecular Medicine Reports provides additional insight into the cellular pathways involved in liraglutide’s adipogenic effects.
Using a series of in vitro experiments, the researchers show that liraglutide does indeed promote the adipogenic differentiation of 3T3-L1 cells (a widely used murine preadipocyte cell line) through a process that upregulates the expression of C/EBPα and PPARγ at the early phase of adipogenic differentiation, promots the expression of lipogenesis associated genes including aP2, and enhances the accumulated of lipids.
At the same time, liraglutide appears to suppress cell proliferation via the Hippo‑yes‑associated protein (YAP) signaling pathway, thereby allowing these cells to transform into mature adipocytes sooner.
How relevant these observations are for humans remains to be seen, but certainly the promotion of adipogenic differentiation may hold the potential for improving insulin sensitivity and reducing the metabolic risks associated with excess weight gain.
@DrSharma
Edmonton, AB
Disclaimer: I have received speaking and consulting honoraria from Novo Nordisk, the maker of liraglutide.
Leptin Induced Lipolysis
 Regular readers will be well aware of leptin as a key hormone secreted by fat tissue.
Regular readers will be well aware of leptin as a key hormone secreted by fat tissue.
Apart from its important role in appetite regulation, leptin has a number of other central and peripheral actions – one of which is to increase activity of the sympathetic nervous system.
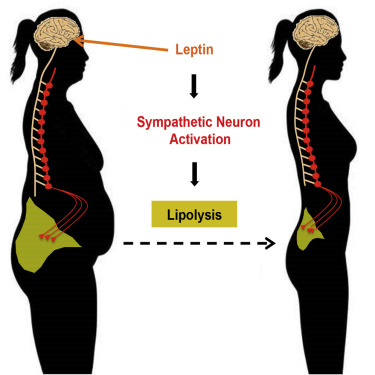
A paper by Wenwen Zeng and colleagues published in Cell, now provides conclusive evidence that leptin can mediate fat breakdown from fat cells and does so via stimulation of the sympathetic nervous system.
Using sophisticated nerve imaging techniques, the researchers show that fat cells are often densely surrounded by sympathetic nerve endings, which, when stimulated, lead to the mobilization of stored fat and a reduction in fat mass.
Genetic ablation of these nerve endings or removal of the key enzyme involved in catecholamine synthesis completely blocks the lipolytic effect of leptin showing that the fat mobilizing effect of leptin is entirely dependent on intact sympathetic innervation and signalling in fat tissue.
Overall the finding that sympathetic nerve activity stimulates lipid release in adipose tissue is not new – but the clear demonstration that his mechanism is harnessed by leptin is.
How this finding could possibly be harnessed for obesity treatment is difficult to say – while stimulating sympathetic nerve activity may well result in lipid mobilisation, it also comes with the feared adverse effects of stimulating heart rate and increasing blood pressure, which would likely limit the clinical use of any such approach.
@DrSharma
Edmonton, AB
An Update On Non-Alcoholic Fatty Liver Disease

Fatty Liver
Of all of the common complications of obesity, fatty liver disease is perhaps the most insidious. Often starting without clinical symptoms and little more than a mild increase in liver enzymes, it can progress to inflammation, fibrosis, cirrhosis and ultimate liver failure. It can also markedly increase the risk for hepatocellular cancer even in patients who do not progress to cirrhosis.
Now, a paper by Mary Rinella from Northwestern University, Chicago, published in JAMA provides a comprehensive overview of what we know and do not know about early detection and management of this condition.
The findings are based on a review of 16 randomized clinical trials, 44 cohort or case-control studies, 6 population-based studies, and 7 meta-analyses.
Overall between 75 million and 100 million individuals in the US are estimated to have nonalcoholic fatty liver disease with 66% of individuals older than 50 years with diabetes or obesity having nonalcoholic steatohepatitis with advanced fibrosis.
Although the diagnosis and staging of fatty liver disease requires a liver biopsy, biomarkers (e.g. cytokeratin 18) may eventually help in the detection of advanced fibrosis.
In addition, non-invasive imaging techniques including vibration-controlled transient elastography, ultrasound with acoustic radiation force impulse or even magnetic resonance elastography are fairly accurate in the detection of hepatic fibrosis and are the most reliable modalities for the diagnosis of advanced fibrosis (cirrhosis or precirrhosis).
Currently, weight loss is the only proven treatment for fatty liver disease. Pharmacotherapy including treatment with vitamin E, pioglitazone, and obeticholic acid may also provide some benefit (none of these treatments currently are approved for this indication by the UD FDA). Futhermore, the potential benefits of existing and emerging anti-obesity treatments on the incidence and progression of fatty liver remains to be established.
As Rinella points out,
“It is important that primary care physicians, endocrinologists, and other specialists be aware of the scope and long-term effects of the disease.”
Clearly, screening for fatty liver disease needs to be part of every routine work up of individuals presenting with excess weight.
@DrSharma
Edmonton, AB
When Identical Twins Are Different

Professor Aila Rissanen, University of Helsinki, Finland
This year’s prestigious Fredrich Wassermann Award of the European Association for the Study of Obesity presented at the 22nd European Congress on Obesity goes to Helsinki’s Aila Rissanen, Europe’s grande dame of obesity research.
I have personally known Aila for as lo as I have been involved in obesity and there is much in her work and approach to obesity that has stimulated my own thoughts on this issue.
In her acceptance address, Aila chose to focus on her work in BMI-discordant twins (among the many topics she has worked on) due to the remarkable insights into the “natre-nurture” discussion that this model offers.
Indeed, it is extremely rare to find genetically identical twins, who differ in body weight (demonstarting just how highly heritable body weight actually is). Thus, body weight in identical twins is remarkably homogeneous not only because of the heritability of weight per se but also due to heritability of weight gain.
Cining the work of her wildly successful trainee Kirsi Pietilainen, Aila described the efforts it took to identify just 30 obesity discordant (weight difference of >10 Kg) identical twins from well over 500 identical twin pairs.
These discordant twin pairs have now been extensively phenotyped with every imaginable laboratory test, measurement and tissue biopsies.
The most consistent difference between the discordant twins appears to be a greater level of physical activity in the leaner twin, which appears to precede the onset of weight gain. In addition to voluntary physical exertion, there also appears to be a significant difference in fidgeting between the twins.
Compared to their co-twins, the obese twins had greater pro-inflammatory lipid profiles, lower antioxident activity and higher pro-coagulation markers. The reasons for these differences remains unclear.
Finally, Aila provided a brief overview of some of the exciting work that is now going on to further study the differences between these genetically identical but obesity disparate twins – metabolomics, lipidomics, epigenomics and even bacteriomics.
Although any of this has yet to translate to better obesity prevention or management, you never know where these fundamental insights into human biology may lead you.
For know, this is certainly a space I intend to watch.
@DrSharma
Prague, Czech Republic
Plan Your Personalized Program For The Canadian Obesity Summit Now
 If you are planning to attend the 4th Canadian Obesity Summit in Toronto next week (and anyone else, who is interested), you can now download the program app on your mobile, tablet, laptop, desktop, eReader, or anywhere else – the app works on all major platforms and operating systems, even works offline.
If you are planning to attend the 4th Canadian Obesity Summit in Toronto next week (and anyone else, who is interested), you can now download the program app on your mobile, tablet, laptop, desktop, eReader, or anywhere else – the app works on all major platforms and operating systems, even works offline.
You can access and download the app here.
(To watch a brief video on how to install this app on your device click here)
You can then create an individual profile (including photo) and a personalised day-by-day schedule.
Obviously, you can also search by speakers, topics, categories, and other criteria.
Hoping to see you at the Summit next week – have a great weekend!
@DrSharma
Gurgaon, Haryana
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
