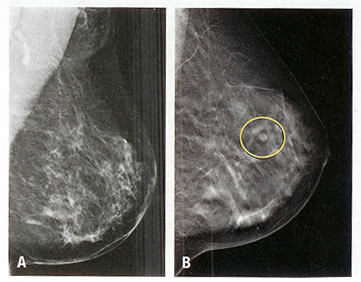
Dose-Response Relationship Between Obesity And Breast Cancer
 With all the concern about the impact of obesity on metabolic and cardiovascular health, it is often forgotten that after smoking, obesity is the single most important risk factor for many common cancers, including of course breast cancer.
With all the concern about the impact of obesity on metabolic and cardiovascular health, it is often forgotten that after smoking, obesity is the single most important risk factor for many common cancers, including of course breast cancer.
The importance of this relationship is again documented by Marian Neuhouser and colleagues in a paper published in JAMA Oncology.
The study examines the associations of overweight and obesity with risk of postmenopausal invasive breast cancer after extended follow-up (about 13 years) in the Women’s Health Initiative (WHI) clinical trials, involving over 67,000 postmenopausal women ages 50 to 79 years at 40 US clinical centers..
Overall, 3388 invasive breast cancers were observed over the follow-up period with women who were overweight or obese having increased risk that was related to their degree of excess weight.
Compared to normal weight women, individuals with Class II and III obesity had a 60% greater risk for invasive breast cancer with an almost 2-fold greater risk for estrogen receptor–positive and progesterone receptor–positive breast cancers.
Class II and III obesity was also associated with a 2-fold greater risk for larger tumor size, positive lymph nodes and deaths.
Furthermore, risk was increased in women with a baseline BMI of less than 25.0 who gained more than 5% of body weight over the follow-up period.
Given this importance of obesity for breast cancer, one can only wonder just how much of the Cancer research funding raised by the Pink Ribbon campaign and other Cancer charities, finds its way into research on obesity treatment and prevention – can’t say I know of any cancer funding that has knocked on the doors of my fellow obesity researchers.
@DrSharma
Edmonton, AB
Childhood Cranial Radiation Therapy May Increase Obesity Risk in Adults
 Among all of the possible factors that may contribute to obesity, one that is seldom discussed (and most people are largely unaware of) is surviving cancer.
Among all of the possible factors that may contribute to obesity, one that is seldom discussed (and most people are largely unaware of) is surviving cancer.
While this is increasingly being appreciated in adults, data on childhood cancer survivors is rather sparse.
Thus, a study by Carmen Wilson and colleagues, published in Cancer, which follows the development of obesity in individuals treated for cancer as kids is of particular interest.
The study looks at 1996 cancer survivors who previously received treatment for cancer at a large Children’s Research Hospital, who survived ≥10 years from diagnosis (median age at diagnosis, 7.2 years; median age at follow-up, 32.4 years).
Interestingly, 47% of survivors, who received cranial radiation therapy developed obesity compared to only 30% of those who did not.
This risk was greatest in those who also received glucocorticoids or were the youngest at the time of treatment.
The researchers also found a significant modifying effect of genetic markers, some of which are known to be involved in neural growth, repair and connectivity.
Thus, this study shows that survivors of childhood cancer appear to be prone to developing obesity as adults particularly if they were treated with cranial radiation therapy and/or corticosteroids.
Clinicians should be aware of this increased risk and should consider measures to prevent excess weight gain in individuals with a history of childhood cancer.
@DrSharma
Edmonton, AB
![]() Wilson CL, Liu W, Yang JJ, Kang G, Ojha RP, Neale GA, Srivastava DK, Gurney JG, Hudson MM, Robison LL, & Ness KK (2015). Genetic and clinical factors associated with obesity among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort. Cancer PMID: 25963547
Wilson CL, Liu W, Yang JJ, Kang G, Ojha RP, Neale GA, Srivastava DK, Gurney JG, Hudson MM, Robison LL, & Ness KK (2015). Genetic and clinical factors associated with obesity among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort. Cancer PMID: 25963547
.
Ten Years of Eating Organic Foods Does Little To Reduce Your Risk of Cancer
![]() There is a widespread belief that conventional use of pesticides, antibiotics and other factors in “industrial” farming may promote the incidence of cancers – a risk that could be avoided by eating “organic”.
There is a widespread belief that conventional use of pesticides, antibiotics and other factors in “industrial” farming may promote the incidence of cancers – a risk that could be avoided by eating “organic”.
According to a paper by Kathryn Bradbury and colleagues, published in the British Journal of Cancer, this may not quite be the case.
The researchers examined prospective data of 620,000 middle-aged UK women on the relationship between the incidence of a variety of cancers and self-reported consumption of organic foods.
Over the 9.3 years of follow-up, there was no relationship between the consumption of organic foods and the incidence of all cancers.
In a subset analyses there was a statistically ‘borderline’ reduction in non-Hodgkin lymphoma, a finding that is perhaps more attributable to statistical chance than to any plausible biological hypothesis.
So, while eating “organic” may have a certain “healthfulness” appeal, a lower risk of cancer may not be a notable benefit.
@DrSharma
Edmonton, AB
![]() Bradbury KE, Balkwill A, Spencer EA, Roddam AW, Reeves GK, Green J, Key TJ, Beral V, & Pirie K (2014). Organic food consumption and the incidence of cancer in a large prospective study of women in the United Kingdom. British journal of cancer PMID: 24675385
Bradbury KE, Balkwill A, Spencer EA, Roddam AW, Reeves GK, Green J, Key TJ, Beral V, & Pirie K (2014). Organic food consumption and the incidence of cancer in a large prospective study of women in the United Kingdom. British journal of cancer PMID: 24675385
.
Does Surviving Breast Cancer Lead to Obesity?
 We have long recognised obesity as significant risk factor for post-menopausal breast cancer but emerging data suggests that surviving cancer may in itself promote weight gain.
We have long recognised obesity as significant risk factor for post-menopausal breast cancer but emerging data suggests that surviving cancer may in itself promote weight gain.
Thus, a study by Rebecca Sedjo and colleagues, in a paper published in the Journal of Cancer Survivorship, notes significant weight gain in 665 overweight and obese women within five years of surviving breast cancer.
The average weight gain over five years was 4.5% with almost half the participants gaining significantly more weight.
Younger women and those with lower BMIs were more likely to gain significant amounts of weight over time.
Pharmacological treatment was also an important predictor of weight gain, with women treated with selective estrogen-receptor modulators twice as likely to gain weight compared to women prescribed aromatase inhibitors.
Clearly, post-diagnosis weight gain is common in breast cancer survivors and is influenced by a complex set of factors including age, ethnicity, weight, smoking status, time elapsed since diagnosis, and endocrine-modulating therapy.
It appears that exploration of effective strategies to prevent this weight gain or provide obesity management strategies to breast cancer survivors are long overdue.
@DrSharma
Edmonton, AB
Clinical Management of Obese Patients With Cancer
Metastasizing Cancer Cell
Obesity is a risk factor for many cancers. But even if this were not the case, the increase in the number of people living with obesity means that more obese people will be diagnosed with cancer than ever before.
The many complex issues facing oncologists in managing their obese cancer patients are nicely summarized and reviewed in a paper by Wenjing Tao and Jesper Lagergren from the Karolinska Institute, Stockholm, Sweden, in a paper published in Nature Reviews Clinical Oncology.
As the authors point out, not only does a large body of epidemiological evidence link obesity to increased cancer incidence, but there is also evidence suggesting poorer survival in obese patients with cancer.
There are also a number of important challenges related to diagnosis including reduced participation of obese individuals in cancer screening programs, lower tumour-marker expression and problems with medical imaging among obese individuals.
Excess body weight also alters pharmacokinetics of chemotherapy and hormone therapy and precision of radiotherapy might be adversely affected by greater skin motility and increased motion of internal organs.
Obese patients can also face higher risks of complications with surgery and recovery times may be affected.
Finally, the authors discuss the importance of sarcopenic obesity and the problem of excess weight gain associated with cancer survival, both of which can affect long-term outcomes.
But, as the authors conclude,
“Although the number of obese patients with cancer is rapidly growing, there is a lack of evidence-based clinical guidelines specifically addressing diagnosis and treatment for these patients.”
@DrSharma
Kananaskis, AB
![]() Tao W, & Lagergren J (2013). Clinical management of obese patients with cancer. Nature reviews. Clinical oncology PMID: 23856746
Tao W, & Lagergren J (2013). Clinical management of obese patients with cancer. Nature reviews. Clinical oncology PMID: 23856746
.
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
