Post-Surgery Weight Regain: Hormonal and Metabolic Factors
Friday, September 13, 2013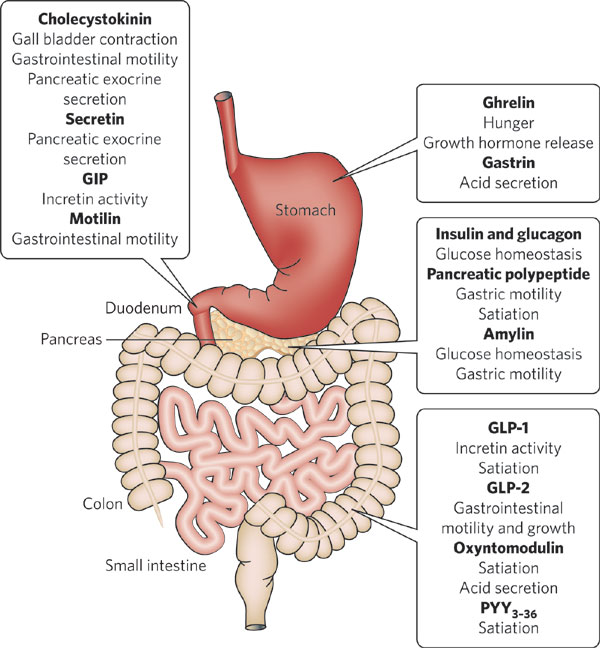 In yesterday’s post, I discussed the importance of dietary factors in weight regain after bariatric surgery.
In yesterday’s post, I discussed the importance of dietary factors in weight regain after bariatric surgery.
In this post, I will discuss the role of hormonal and metabolic factors identified in our systematic review of post-surgical weight regain published in Obesity Surgery.
It is now widely assumed that the efficacy of bariatric surgery is not solely dependent on causing a “restriction” or simply “malabsorbtion” of calories.
Rather, there is now growing consensus that the key reason why bariatric surgery works is through its impact on gut hormones and neurological signals from the gut that significantly reduce hunger and/or satiety.
Thus, it is not surprising that in our review we found several studies that noted a significant relationship between post-surgical levels of the “hunger hormone” ghrelin and post-surgical weight regain. Patients who experienced less weight loss or greater weight regain after sleeve gastrectomy and/or roux-en-y bypass surgery demonstrated higher fasting and post-prandial ghrelin levels. Elevated ghrelin levels were also found to correlate with a return of hunger in patients with regain.
Other evidence points to the role of hypoglycaemia in promoting weight regain in some patients. Reactive hypoglycaemia after bariatric surgery may result from the rapid transit of ingested carbohydrates into the small intestine thereby generating an early and significant insulin surge which results in a reactive hypoglycaemia shortly after a meal. This would in turn prompt snacking and increased caloric ingestion resulting in weight regain.
While there is currently no medical treatment to deal with ghrelin elevations, the latter problem can potentially be managed by dietary measures, including the avoidance of high-glycemic index foods.
Given that there are many gut hormones that may be altered by bariatric surgery and their individual roles are still poorly understood, it is clear that we will need further studies to better understand how these factors may explain why some patients failure to lose weight after surgery or show a greater tendency for weight regain.
@DrSharma
Chicago, IL
![]()
Karmali S, Brar B, Shi X, Sharma AM, de Gara C, & Birch DW (2013). Weight Recidivism Post-Bariatric Surgery: A Systematic Review. Obesity surgery PMID: 23996349
.

