Post-Bariatric Surgery Vitamins and Minerals
Tuesday, November 4, 2014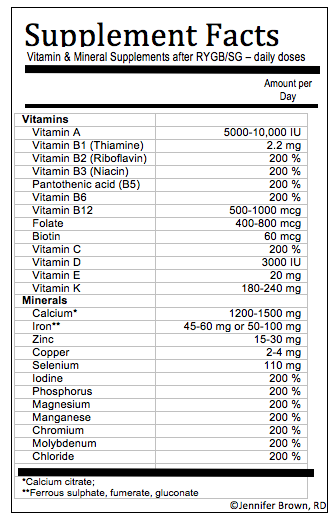 Last week, at the 4th Dietitian Obesity Learning Retreat, co-hosted by the Canadian Obesity Network and Dietitians Canada, Jennifer Brown, co-chair of the Ontario Bariatric Network Dietitian Task Force creator of the bariatric surgery subgroup of the Dietitians of Canada – Diabetes Obesity and Cardiovascular network, presented a neat little nutrition label-style compilation of the essential vitamin and mineral requirements for post-bariatric surgery patients.
Last week, at the 4th Dietitian Obesity Learning Retreat, co-hosted by the Canadian Obesity Network and Dietitians Canada, Jennifer Brown, co-chair of the Ontario Bariatric Network Dietitian Task Force creator of the bariatric surgery subgroup of the Dietitians of Canada – Diabetes Obesity and Cardiovascular network, presented a neat little nutrition label-style compilation of the essential vitamin and mineral requirements for post-bariatric surgery patients.
Jennifer has been a Registered Dietitian with The Ottawa Hospital Weight Management Clinic and Bariatric Centre of Excellence since 2007 and is currently pursuing her Master’s at the University of Ottawa; exploring the relationship between appetite, smell performance and peripheral hormone changes after Roux-en-Y gastric bypass surgery. Jennifer was recently nominated to the American Academy of Nutrition and Dietetics Evidence Analysis Workgroup on Bariatric Surgery and was a national recipient of the Dietitians of Canada Graduate Award and national recipient of the 2014 Rebecca Snowball Reeves Award from the American Academy of Nutrition & Dietetics. She has specialized training in bariatric nutrition from the Edmonton Weight Wise program, ASMBS, The Obesity Society, the Canadian Obesity Network and the International Association for the Study of Obesity.
Jennifer hopes to standardize bariatric nutrition care and collaborate on nutrition-related research across Canada and internationally.
Jennifer can be contacted through the Canadian Obesity Network.
@DrSharma
Boston, MA

