How Well Is Cardiometabolic Risk Being Managed in Primary Care?
Tuesday, March 12, 2013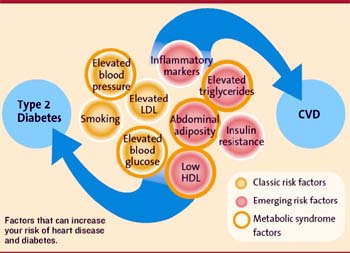 “Cardiometabolic” is a term that is often used (often synonymous with “metabolic syndrome”) to describe the constellation of cardiovascular risk factors (many of which happen to be metabolic).
“Cardiometabolic” is a term that is often used (often synonymous with “metabolic syndrome”) to describe the constellation of cardiovascular risk factors (many of which happen to be metabolic).
A study by Teoh and colleagues from across Canada, published in the Canadian Journal of Cardiology, examined risk assessment and management patterns by primary care physicians, working both in primary care teams (PCT) and in solo practice.
Based on an analysis of almost 2,500 patients (40 years old with no clinical evidence of cardiovascular disease and diagnosed with at least 1 of the following: dyslipidemia, type 2 diabetes mellitus (T2DM), or hypertension.), most (~90%) were abdominally obese and at least 52.2% had metabolic syndrome.
Cardiovascular risk, was often miscalculated and behavioural modification was recommended in fewer than 50% of patients (compared to pharmacotherapy in >70%).
Overall, guideline-recommended control of cardiometabolic risk factors was achieved in only about 10% of patients.
Not surprisingly, the authors are not happy about how obesity and cardiovascular risk is currently being assessed in primary care and call for a paradigm change in assessing and managing obesity and cardiovascular risk with more aggressive lifestyle interventions.
While this is certainly a laudable goal, there is ample evidence that simply telling people to “eat-less-move-more” is not the answer. In fact, even simply putting more allied health into these teams may also not be the answer.
As the authors note,
“We found that evidence for exercise and nutrition counselling aimed at encouraging sustained negative energy balance was disappointingly infrequent. This was surprising because 5 PCTs had a diabetes educator and 7 had a dietitian on staff or as part of the extended care program.”
In fact, it was particularly surprising to note that,
“Management of CMR factors appeared to be no more effective in PCTs compared with the more traditional Solo practices.”
Thus, the paradigm shift is probably not so much in recognising the importance of “lifestyle” interventions but rather in their delivery – so far I have yet to see a successful sustainable delivery model outside of the rather artificial constraints of clinical intervention trials that demonstrate “successful” lifestyle management.
This is not to say that “lifestyle” interventions cannot significantly improve cardiometabolic risk factors. However, the effort to achieve and maintain these changes in clinical practice in enough patients to make a significant impact on outcomes is generally underestimated.
Not to say that such a model may not not exist in some corner of the earth – it is just that most health systems have yet to figure out how to do this.
AMS
Edmonton, AB
![]() Teoh H, Després JP, Dufour R, Fitchett DH, Goldin L, Goodman SG, Harris SB, Langer A, Lau DC, Lonn EM, John Mancini GB, McFarlane PA, Poirier P, Rabasa-Lhoret R, Tan MK, & Leiter LA (2013). Identification and Management of Patients at Elevated Cardiometabolic Risk in Canadian Primary Care: How Well Are We Doing? The Canadian journal of cardiology PMID: 23465284
Teoh H, Després JP, Dufour R, Fitchett DH, Goldin L, Goodman SG, Harris SB, Langer A, Lau DC, Lonn EM, John Mancini GB, McFarlane PA, Poirier P, Rabasa-Lhoret R, Tan MK, & Leiter LA (2013). Identification and Management of Patients at Elevated Cardiometabolic Risk in Canadian Primary Care: How Well Are We Doing? The Canadian journal of cardiology PMID: 23465284

