Durability of Diabetes Remission After Bariatric Surgery
Tuesday, September 8, 2015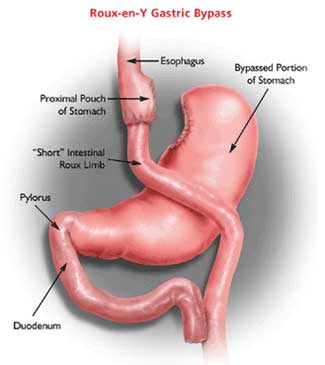 There is no doubt that for the vast majority of patients with type 2 diabetes, bariatric (or, as some surgeons prefer to call it, “metabolic”) surgery, can lead to marked improvement and even remission of diabetes.
There is no doubt that for the vast majority of patients with type 2 diabetes, bariatric (or, as some surgeons prefer to call it, “metabolic”) surgery, can lead to marked improvement and even remission of diabetes.
A paper published in The Lancet by Geltrude Mingrone and colleagues, shows that even five years following surgery, about 50% of patients who had a biliopancreatic diversion (a rather uncommon and somewhat drastic form of bariatric surgery) and about 40% of patients who had a roux-n-y gastric bypass will still be in remission.
No doubt (as the study shows), such results are unthinkable with conventional treatments.
Although numbers are small, the fact that 25% of the non-surgical patients in this study experienced major complications from their diabetes, compared to none in the surgical groups, suggests that this is not simply glucose cosmetics but rather, that the metabolic benefits of surgery do turn into tangible benefits.
So what does this mean for the diabetes epidemic – not much, I’m afraid.
Not because surgery is not effective – it surely is.
Unfortunately, however, surgery is not scalable the way medical treatments are.
Even if we magically saw a three-fold increase in bariatric surgery (to worldwide about 1 million surgeries a year), this would hardly make a noticeable dent in the prevalence (or for that matter complications) of over 400 million people living with diabetes.
Even a five or ten-fold increase in metabolic surgery would hardly be noticeable at a global level.
Bariatric surgery (as most surgeries), is simply not a scalable procedure for a disease that affects 15% or more of the population.
Thus, aside from helping the lucky few, who do somehow manage to get surgery, the real lesson here is that we urgently need to understand exactly why surgery works (it is not just weight loss, although this does contribute to the benefit).
There are many things that happen after surgery – changes in hormonal responses to food intake (e.g. higher levels of GLP-1), changes in gut microbiota, changes in bile acid metabolism). We need to understand these factors and find non-surgical ways to mimic these changes in a manner that allows scalability to millions of people around the world.
This does not mean we need to stop doing surgery – rather, the more patients can benefit from this treatment now, the better (for them).
But let us not kid ourselves that surgery will one day solve the problem – till we can package the metabolic benefits of surgery into a tablet or a pen (or both), these findings will have little impact on the global problem of diabesity.
@DrSharma
Edmonton, AB

