Disease Severity and Staging of Obesity
Wednesday, October 15, 2014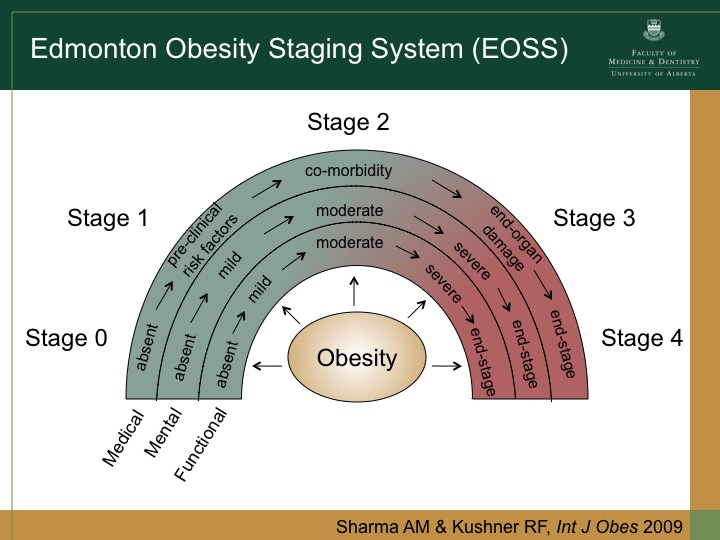 Regular readers will be well aware of our work on the Edmonton Obesity Staging System (EOSS), that classifies individuals living with obesity based on how “sick” rather than how “big” they are.
Regular readers will be well aware of our work on the Edmonton Obesity Staging System (EOSS), that classifies individuals living with obesity based on how “sick” rather than how “big” they are.
For a rather comprehensive review article on the issue of determining the severity of obesity and potentially using this as a guide to treatment, readers may wish to refer to a paper by Whyte and colleagues from the University of Surrey, UK, published in Current Atherosclerosis Reports.
This paper not only nicely summarizes the potential effects of obesity on various organs and organ systems but also discusses the use of staging systems (EOSS and Kings) as a way to better characterize the impact of excess weight on an individual.
As the authors note in their summary,
“Using a holistic tool in addition to BMI allows highly informed decision-making and on a societal level helps to identify those most likely to gain and where economic benefit would be maximised.”
Not surprisingly, the Edmonton Obesity Staging System, which has been validated against large data sets as a far better predictor of mortality than BMI, waist circumference or metabolic syndrome, is being increasingly adopted as a practical tool to guide clinical practice.
@DrSharma
Merida, Mexico
![]() Whyte MB, Velusamy S, & Aylwin SJ (2014). Disease severity and staging of obesity: a rational approach to patient selection. Current atherosclerosis reports, 16 (11) PMID: 25278281
Whyte MB, Velusamy S, & Aylwin SJ (2014). Disease severity and staging of obesity: a rational approach to patient selection. Current atherosclerosis reports, 16 (11) PMID: 25278281

