Are There Merits To Subtyping Obesity?
Wednesday, December 11, 2013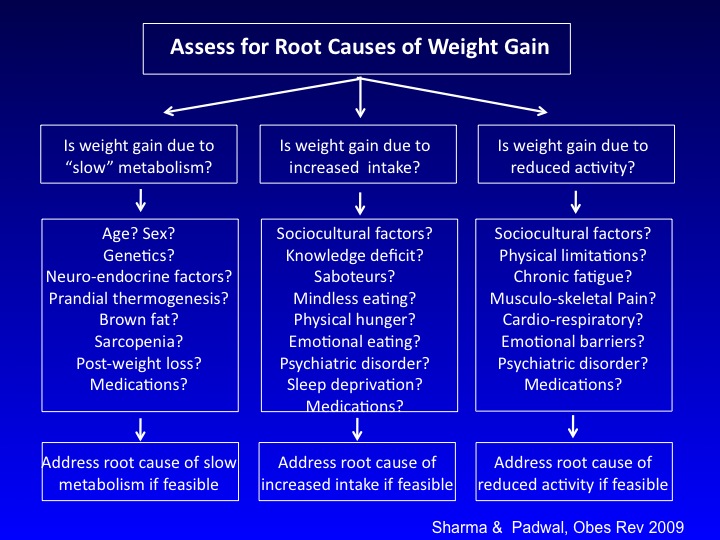 Regular readers may recall that several years ago we proposed that it was time to move beyond considering obesity a homogeneous entity (as defined by BMI alone) and suggested that clinicians may be better off using an “etiological framework” for assessing and addressing the diversity of factors that drive weight gain.
Regular readers may recall that several years ago we proposed that it was time to move beyond considering obesity a homogeneous entity (as defined by BMI alone) and suggested that clinicians may be better off using an “etiological framework” for assessing and addressing the diversity of factors that drive weight gain.
This notion, that obesity is not a homogeneous condition, is something other researchers are now slowly catching up with.
One example of how “mainstream” thinking is gradually embracing the concept of heterogeneity in obesity is a recent paper by Allison Field and colleagues from Harvard Medical School published in JAMA.
In this paper the authors state that,
“One reason for the lack of stronger associations with risk factors or more consistently successful treatment is that all types of overweight and obesity are often grouped together. This approach potentially obscures strong associations between risk factors and specific subtypes of obesity.”
This is a problem that we have long lamented and regular readers will be well aware that this was the very basis for developing the Edmonton Obesity Staging System (EOSS) as a way to classify obese patients based on how “sick” they are rather than just on how “big” they are.
While the authors of this paper may yet have to familiarize themselves with the literature on this issue, there is certainly no reason to expect why individuals with higher EOSS stages will not be the ones to benefit more from obesity interventions than those in the low-risk groups.
Depite making a few good points about advances in molecular epidemiology, this article lacks sharp thinking in that it does not clearly distinguish between “etiological” and “phenotypic” heterogeneity of obesity.
While the former applies to the many drivers of obesity (which we have categorized as predominantly affecting metabolism, ingestive behaviour and/or physical activity), the latter applies to the many consequences of obesity (which we have categorized as affecting physical, mental and functional health).
As we have previously pointed out, the two are not necessarily related.
Thus, two individuals, gaining weight for entirely different reasons (e.g. food insecurity vs. binge-eating syndrome), may well present with exactly the same amount of excess body fat and identical clinical complications (e.g. diabetes, reflux disease and urinary incontinence).
On the other hand, two individuals, gaining weight for exactly the same reason (e.g. on anti-psychotic medications), may present with quite different complications (e.g. sleep apnea vs. osteoarthritis).
Thus, while ‘subtyping’ of obesity at the molecular or genetic level (as suggested by the authors), may well be of interest, there are already clinically meaningful ways to subtype obese individuals both with regard to etiology and clinical risk.
Nevertheless, the authors are certainly correct in their statement that,
“Obesity is a heterogeneous and complex disease influenced by exogenous and endogenous exposures. Stratifying obesity into meaningful subtypes could provide a better understanding its causes and enable the design and delivery of more effective prevention and treatment interventions.”
It is good to see “mainstream” thinking on this issue finally catching up with this concept.
@DrSharma
Berlin, Germany
![]() Field AE, Camargo CA Jr, & Ogino S (2013). The merits of subtyping obesity: one size does not fit all. JAMA : the journal of the American Medical Association, 310 (20), 2147-8 PMID: 24189835
Field AE, Camargo CA Jr, & Ogino S (2013). The merits of subtyping obesity: one size does not fit all. JAMA : the journal of the American Medical Association, 310 (20), 2147-8 PMID: 24189835
.

