How To Make Obesity Healthcare Teams Work
Wednesday, February 3, 2016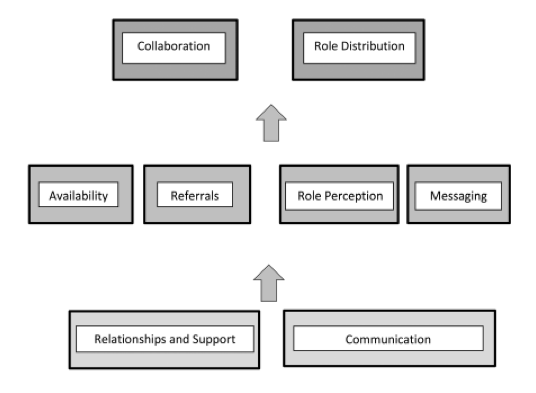
Interaction between key patterns regarding interdisciplinarity in patient weight management.
Obesity, like most other chronic diseases, requires interdisciplinary approaches that involves a wide range of clinicians from different disciplines (e.g. physician, nurse, psychologist, dietitian, exercise physiologist, social worker, physiotherapist, occupational therapist, etc.).
But exactly how to get these teams to function efficiently and deliver timely and ongoing obesity management remains largely understudied.
In a paper by Jodi Asselin and colleagues, published in Clinical Obesity, we explore the challenges faced by members of multidisciplinary teams working in the setting of a large primary care network.
Participants (n = 29) included in this analysis are healthcare providers supporting chronic disease management in 12 family practice clinics randomized to the intervention arm of the 5As Team trial including mental healthcare workers (n = 7), registered dietitians (n = 7), registered nurses or nurse practitioners (n = 15). Participants were part of a 6-month intervention consisting of 12 biweekly learning sessions aimed at increasing provider knowledge and confidence in addressing patient weight management.
Qualitative methods included interviews, structured field notes and logs.
Four common themes of importance in the ability of healthcare providers to address weight with patients within an interdisciplinary care team emerged, (i) Availability; (ii) Referrals; (iii) Role perception and (iv) Messaging.
Availability (i) refers to the ability of two or more people to meet and communicate as needed within a reasonable amount of time. This included the interdisciplinary team members knowing and meeting each other, being able to consistently communicate during the work-day, or deliberately asynchronously, and having work schedules that allowed collaboration.
Availability was often affected by scheduling that limited face-to-face time between providers and subsequently limited the potential for collaboration or discussion. Another issue was lack of in-clinic time to speak to providers who were physically present but otherwise unavailable.
Referrals (ii) points to the need for weight management referrals to take place, for those referrals to be appropriate to provider ability and for the patient to be knowledgeable about, or in agreement with the reason for referral. Many practitioners felt they were not receiving the weight management referrals they could, or that the referrals often left the patient and provider unclear as to where to begin the conversation.
Role perception (iii) concerns the way a provider’s role is understood by other interdisciplinary team members. Issues pertaining to role perception were fairly consistent and strongly linked to concerns with referrals. Common examples included concern that they were not receiving the type of referrals they could, that other providers did not understand their role in weight management, or that they as providers did not understand the role of others.
Messaging (iv) refers to the overall approach to weight management that providers within the same clinic were using, as well as the key information being shared between providers and patients. Inconsistent messaging among providers within clinics, as well as with specialists seen by the patient, was a common concern raised during interviews. In such cases there was feeling that advice was not patient-centred, that efforts had not been taken to consider patient history and that as a consequence, the patient might suffer a setback, reduced interest, or reduced personal confidence. In these cases the message a patient had received from another provider was counter to the message or approach the interviewee was giving.
However, we find that what was key to our participants was not that these issues be uniformly agreed upon by all team members, but rather that communication and clinic relationships support their continued negotiation.
Our study shows that firm clinic relationships and deliberate communication strategies are the foundation of interdisciplinary care in weight management.
Furthermore, there is a clear need for shared messaging concerning obesity and its treatment between members of interdisciplinary teams.
From the project it is evident that broad training in the various contributors to obesity enables providers to not only see their own role in treatment, but to better understand the role of others and therefore begin addressing problems in referrals, messaging and role perception.
@DrSharma
Edmonton

