Factors Affecting Ingestive Behaviour: Physiological or Homeostatic Factors
Thursday, June 28, 2018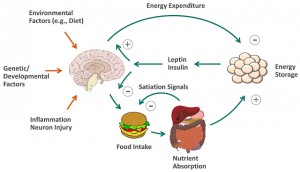 Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour:
Continuing with citations from my article in Obesity Reviews on an aeteological framework for assessing obesity, we now turn to the some of the factors that can affect ingestive behaviour:
Physiological or Homeostatic Factors
In contrast to excess caloric consumption that results largely from environmental determinants, over‐eating in response to increased hunger or reduced satiety can be viewed as a physiological response to a perturbation of the homeostatic system and is perhaps best termed homeostatic hyperphagia. Primary homeostatic hyperphagia can result from genetic defects in the homeostatic system (e.g. leptin deficiency, melanocortin type 4 receptor mutation or Prader Willi Syndrome) and are rare. Secondary homeostatic hyperphagia can result from acquired defects or perturbations in the homeostatic system (e.g. head trauma, craniopharyngeoma, insulinoma). Tertiary homeostatic hyperphagia, by far the most common category, is largely the result of inappropriate feeding intervals and/or nutrient selection. Thus, skipping meals, resulting in a compensatory hyperphagic response (rapid ingestion of energy‐dense foods), is perhaps the most prevalent form of homeostatic hyperphagia. Ingestion of high‐glycemic foods resulting in a rapid rise and fall in blood glucose and insulin levels (‘crash and crave’) may prompt increased snacking and overconsumption, although this notion remains controversial. Meal duration and composition can also affect satiety response, whereby delayed or reduced satiation (e.g. in response to hasty eating, energy‐dense foods, low fibre intake, liquid calories) can result in excess caloric intake. The presence of homeostatic hyperphagia (characterized by over‐eating in response to increased hunger and/or reduced satiety) will likely call for interventions that specifically address the underlying perturbation in this system (e.g. administration of leptin, excision of the insulinoma, correction of meal pattern, nutritional hygiene, portion control, etc.). Patients with obesity resulting from tertiary homeostatic hyperphagia are the most likely to benefit from dietary counselling.
@DrSharma
Edmonton, AB

