My Talks At The 2015 Minimally Invasive Surgery Symposium
 This week I will be giving a key note address on the use of the Edmonton Obesity Staging System (and the shortcomings of BMI) at the 2015 Minimally Invasive Surgery Symposium (MISS) in Las Vegas.
This week I will be giving a key note address on the use of the Edmonton Obesity Staging System (and the shortcomings of BMI) at the 2015 Minimally Invasive Surgery Symposium (MISS) in Las Vegas.
Without doubt, minimally invasive laparoscopic surgery has revolutionised bariatric surgery – what was once a messy, life-threatening operation is now an elegant procedure, which usually has patients up and about the next day.
But are the BMI-based indications for bariatric surgery still the best way to go? Not when we have better systems like the Edmonton Obesity Staging System (EOSS) to determine how “sick” someone is rather than just how “big”.
This morning, in a separate presentation, I will also be providing an extensive overview on the efficacy and safety of the modern anti-obesity medications that have recently become available in the US.
While these medications may still not help patients achieve or maintain quite the degree of weight loss seen with surgery, they are certainly viable treatment options for individuals with less severe obesity or those unwilling or unable to undergo surgery.
Although evidence for this is still scarce, these medications may well also come to play a role in helping prevent the weight gain that some patients experience after surgery.
If nothing else, minimally invasive bariatric surgeons should certainly be aware of the available medical treatments as they counsel their patients about the pros and cons of surgery.
@DrSharma
Las Vegas, NV
Early Bird Registration For Canadian Obesity Summit Ends March 3rd
For all my Canadian readers (and any international readers planning to attend), here just a quick reminder that the deadline for early bird discount registration for the upcoming 4th Canadian Obesity Summit in Toronto, April 28 – May 2, ends March 3rd.
To anyone who has been at a previous Canadian Summit, attending is certainly a “no-brainer” – for anyone, who hasn’t been, check out these workshops that are only part of the 5-day scientific program – there are also countless plenary sessions and poster presentations – check out the full program here.
Workshops:
Public Engagement Workshop (By Invitation Only)
Pre-Summit Prep Course – Overview of Obesity Management ($50)
Achieving Patient‐Centeredness in Obesity Management within Primary Care Settings
Obesity in young people with physical disabilities
CON-SNP Leadership Workshop: Strengthening CON-SNP from the ground up (Invitation only)
Exploring the Interactions Between Physical Well-Being and Obesity
Intergenerational Determinants of Obesity: From programming to parenting
Neighbourhood Walkability and its Relationship with Walking: Does measurement matter?
The EPODE Canadian Obesity Forum: Game Changer
Achieving and Maintaining Healthy Weight with Every Step
Adolescent Bariatric Surgery – Now or Later? Teen and provider perspectives
Promoting Healthy Maternal Weights in Pregnancy and Postpartum
Rewriting the Script on Weight Management: Interprofessional workshop
Paediatric Obesity Treatment Workshop (Invitation only)
Balanced View: Addressing weight bias and stigma in healthcare
Drugs, Drinking and Disordered Eating: Managing challenging cases in bariatric surgery
From Mindless to Mindful Waiting: Tools to help the bariatric patient succeed
Getting Down to Basics in Designing Effective Programs to Promote Health and Weight Loss
Improving Body Image in Our Patients: A key component of weight management
Type 2 Diabetes in Children and Adolescents: A translational view
Weight Bias: What do we know and where can we go from here?
Innovative and Collaborative Models of Care for Obesity Treatment in the Early Years
To register – click here.
@DrSharma
Edmonton, AB
EOSS Features Prominently in The Lancet’s Obesity Management Recommendations
 It would hardly come as a surprise to regular readers that I would be delighted to see the Edmonton Obesity Staging System featured quite prominently in the article on obesity management by Dietz and colleagues in the 2015 Lancet series on obesity.
It would hardly come as a surprise to regular readers that I would be delighted to see the Edmonton Obesity Staging System featured quite prominently in the article on obesity management by Dietz and colleagues in the 2015 Lancet series on obesity.
Here is what the article has to say about EOSS:
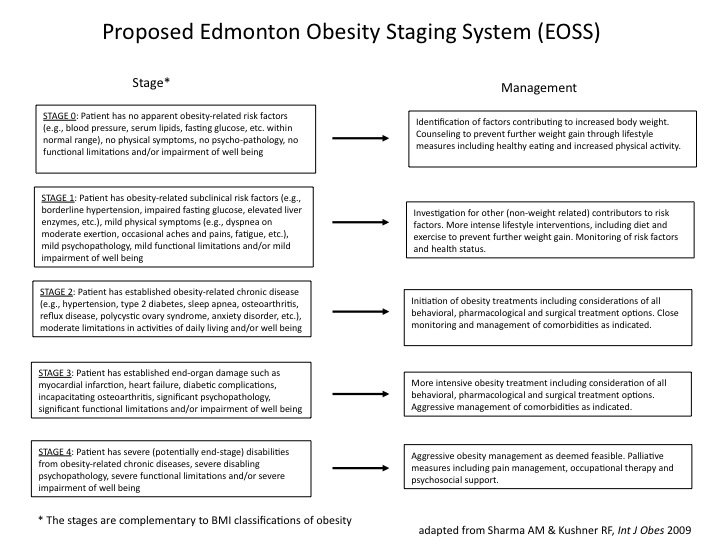
“The Edmonton obesity staging system (EOSS) has been used to provide additional guidance for therapeutic interventions in individual patients (table 1). EOSS provides a practical method to address the treatment paradigm. In principle, EOSS stages 0 and 1 should be managed in a community and primary care setting. Recent data from the USA suggest that 8% of patients with severe obesity (BMI ≥35 kg/m²) account for 40% of the total costs of obesity, whereas the more prevalent grade 1 obesity accounts for a third of costs. These findings suggest that greater priority should be accorded to EOSS stages 3 and 4, resulting in greater focus on pharmacological and surgical management delivered in specialist centres.”
These recommendations are not surprising, as EOSS was specifically designed to provide a much better representation of how “sick” a patient is rather than just how “big” she is.
This is why EOSS has now found its way not just into the 5As of Obesity Management framework of the Canadian Obesity Network but also into the treatment algorithm of the American Society of Bariatric Physicians.
To download a slide presentation on how EOSS works click here.
@DrSharma
Edmonton, AB
Health Professionals’ Weight Bias Does Not Help
 Yesterday, I discussed the dire need for health professional education in obesity, a topic of keen interest to Bill Dietz and colleagues in their paper in the 2015 Lancet series on obesity.
Yesterday, I discussed the dire need for health professional education in obesity, a topic of keen interest to Bill Dietz and colleagues in their paper in the 2015 Lancet series on obesity.
This lack of professional training in obesity is not helped by the well known and widespread weight-bias and discrimination that is rampant amongst most health providers, administrators and policy makers (not to mention the general public).
Thus,
“Weight bias by preclinical and medical students includes attitudes that patients with obesity are lazy, non-compliant with treatment, less responsive to counselling, responsible for their condition, have no willpower, and deserve to be targets of derogatory humour, even in the clinical-care environment. These biases can also lead to views that obesity treatment is futile and feelings of discomfort, which students report as a barrier to discussing weight with patients, both of which are likely to impair care.”
These attitudes have real consequences for people living with obesity,
“Providers spend less time in appointments, provide less education about health, and are more reluctant to do some screening tests in patients with obesity. Furthermore, physicians report less respect for their patients with obesity, perceive them as less adherent to medications, express less desire to help their patients, and report that treating obesity is more annoying and a greater waste of their time than is the treatment of their thinner patients”
It should come as no surprise that patients who experience these attitudes are less likely to seek medical care, even when needed,
“Among the heaviest women, 68% reported delaying use of health-care services because of their weight, due to previous experiences of disrespectful treatment from health-care providers, embarrassment about being weighed, and medical equipment that was too small for their body size.”
This not only directly harms patients but also substantially adds to the cost of the disease as the delay in diagnosis and treatment for obesity-related comorbidities can impair the quality of care for individuals with obesity.
However, these challenges are not insurmountable,
“Information about obesity that indicates contributing factors beyond personal control (eg, biological and genetic contributors) as well as the difficulties in obtaining clinically significant and sustainable weight loss, has been shown to reduce negative bias and stereotypes among preclinical and medical students and improve self efficacy for counselling patients with obesity.”
This is why the Canadian Obesity Network has made addressing weight bias and discrimination its #1 priority in all educational activities geared to health professionals and decision makers.
As long as we basing our discussion of obesity prevention and treatment on unhelpful and harmful stereotypes, we will not be helping the people who actually have the problem.
@DrSharma
Edmonton, AB
Health Professionals Are Poorly Prepared To Address Obesity
“…health professionals are poorly prepared to address obesity. In addition to biases and unfounded assumptions about patients with obesity, absence of training in behaviour-change strategies and scarce experience working within interprofessional teams impairs care of patients with obesity.“
This quote, taken from the paper by William Dietz and colleagues included in the 2015 Lancet series on obesity, pretty sums up the dire state of affairs when it comes to health professionals’ ability to help people living with obesity.
While governments around the world continue to dither on prevention measures, and even if these were implemented, would take decades to substantially reduce global obesity rates (a halting in progression would already be widely considered a major success), health care systems the world around are challenged with an enormous clinical burden that will require innovative treatment and care-delivery strategies are needed.
Well, not all that innovative – after all, the very same health care systems are well versed with providing ample care for scores of other chronic diseases – obesity is just not one of them.
As Dietz points out,
“Existing shortcomings of current health-service delivery include poor teamwork, a mismatch of competencies to the needs of patients and populations, episodic rather than continuous care, and hyperspecialisation.”
In fact we don’t even know if health professionals are actually being trained for this at all,
“A scarcity of information exists for undergraduate medical education in obesity, and even less information is available for nursing and allied health professional students.”
Despite various high-sounding recommendations,
“Overall, the level of implementation of health professional education in obesity at all levels appears inadequate in several countries….The Royal Australian College of General Practitioners is the only specialist training college to include obesity in the prescribed curriculum.”
In Canada we are still licensing family physicians without any requirement to have spend even a single day in a bariatric centre. The recently released Canadian Obesity Practice Guidelines, endorsed by the Canadian College of Family Physicians, provide virtually no guidance to family doctors apart from the rather strong recommendation (based on virtually non-existent evidence) to record BMIs on all patients.
According to Dietz,
“Commonly identified areas for additional training in the care of adults with obesity include motivational interviewing, the comanagement of bariatric surgery patients, and nutrition and exercise counselling.”
Clearly, the emerging role of pharmacotherapy will add a further dimension to the need for health professional education.
None of this will happen without also addressing the stigma and bias against people presenting with excess weight continue to face in their dealing with health professionals. More on this in tomorrow’s post.
@DrSharma
Edmonton, AB
Watch Dr. Sharma in the News!

Listen to Dr. Sharma!
